The former chair of the now-disbanded Jan. 6 committee introduced a bill Friday that would strip Secret Service protection of any former executive convicted of a felony — an effort to avoid the complications of incarcerating formerPresident Trump should he be ordered to serve jail time.
Dubbed the “Denying Infinite Security and Government Resources Allocated toward Convicted and Extremely Dishonorable (DISGRACED) Former Protectees Act,” the legislation from Rep. Bennie Thompson (D-Miss.) would nix the lifelong protection given to former presidents if they are convicted and sentenced for a felony that carries a year or more in prison time.
“Unfortunately, current law doesn’t anticipate how Secret Service protection would impact the felony prison sentence of a protectee — even a former President,” Thompson said in a statement.
“It is regrettable that it has come to this, but this previously unthought-of scenario could become our reality. Therefore, it is necessary for us to be prepared and update the law so the American people can be assured that protective status does not translate into special treatment — and that those who are sentenced to prison will indeed serve the time required of them.”
The move takes aim at Secret Service protections that have left some legal observers suggesting that any eventual conviction of Trump would likely spur some form of home confinement rather than prison time, given his round-the-clock protection.
“This bill would remove the potential for conflicting lines of authority within prisons and allow judges to weigh the sentencing of individuals without having to factor in the logistical concerns of convicts with Secret Service protection,” Thompson’s team wrote on a one-pager on the bill.
Secret Service protections are not just afforded to current and former presidents but also other high ranking officials and immediate family members of protectees.
But Trump is the only protectee facing felony charges — 91 various felony charges across four different state and federal cases.
Trump is currently in court in New York in his hush money trial and is facing charges related to Jan. 6 in federal court in Washington and in Georgia. His federal documents case is being overseen in Florida.
Thompson also claims the bill does not raise ex post facto concerns — those raised when a law is applied retroactively — citing case law finding the government can strip benefits so long as the change was not found to have an “unlawful, punitive purpose.”
Contractors for the Centers for Medicare and Medicaid Services (CMS) cut access to tests for transplant patients that could show early signs of organ rejection despite expert physicians advising the opposite, a new report has found.
The Health Equity in Transplantation Coalition (HEiTC) announced Friday that a Freedom of Information Act request found that Medicare contractors limited access to blood tests even after the recommendations given by the government-chosen panel of medical experts.
Al B. Sure!, executive chairman of HEiTC, said he was “incredibly alarmed” by the findings.
“Instead of listening to these experts and considering what these tests meant to tens of thousands of transplant recipients, the contractor not only ignored but withheld their expert opinion,” he said. “In the process, they took away a vital tool for other doctors to monitor an overwhelmingly Black and Brown transplant community, which for the last year has lived with more anxiety than they should.”
“It’s never been more important that these cutbacks are reversed and coverage without any tie to a biopsy is restored,” he added.
The FOIA request detailed that contractors failed to disclose and then ignored the near-unanimous advice of expert physicians, who were picked by the contractors, to evaluate the utility for tests that could detect early signs of organ rejection in organ transplant recipients without a biopsy.
Five out of six experts testified in November 2022 that such testing had significant clinical benefits, including for routine testing.
But in March 2023, the contractor issued a new “billing article” that dramatically cut Medicare coverage on such tests. Instead, transplant recipients who rely on the federal health insurance program can only access these noninvasive tests for routine surveillance in lieu of a biopsy.
This, HEiTC argues, significantly compromises the ability to catch organ rejection before it actually happens.
The coalition, which was founded by music artist Al B. Sure! and the Rev. Al Sharpton following the billing article, said the change disproportionately affected Black and Brown transplant recipients.
Black, Hispanic and Latino Americans account for 40 percent of transplant recipients in the nation, according to the coalition. They also make up 50 percent of those on the 100,000-person transplant waiting list.
But the issue has become bipartisan, with 14 members of the House, led by Reps. Anna Eshoo (D-Calif.) and Michael Burgess (R-Texas), sending a letter of concern to CMS about the rollbacks.
A follow-up letter was sent in October, and just this month, more than two dozen leading transplant clinicians sent a letter to CMS Administrator Chiquita Brooks-LaSure.
The clinicians detailed the negative impacts of the policy change, including rise in rejection events among organ transplant recipients, which they believe to be associated with the restrictions.
CMS will spend the next few weeks determining whether the cutbacks will remain permanent.
UnitedHealth CEO Andrew Witty will testify in front of a House oversight panel next month about the massive cyberattack on Change Healthcare, as Congress grapples with the fallout and lawmakers’ response.
The May 1 hearing at the House Energy and Commerce oversight subcommittee will mark the first time Witty appears in the House. The panel’s health subcommittee held a hearing this week about the hack, but no representatives from United testified.
“Americans are still dealing with the fallout of the Change Healthcare hack. Individuals and smaller providers, in particular, have struggled financially following the cyberattack, threatening critical access for patients,” Energy and Commerce Committee Chair Cathy McMorris Rodgers (R-Wash.) and oversight subcommittee chair Morgan Griffith (R-Va.) said in a joint statement Friday.
“While we’re disappointed that UnitedHealth could not join us for the recent Health Subcommittee hearing on cybersecurity, we look forward to learning more on what happened in the lead up to, and in the weeks following, the attack,” the lawmakers said.
Change Healthcare is the country’s largest medical claims processor, serving as a sort of clearinghouse of data for health insurers and providers. February’s cyberattack sent shockwaves through the whole health industry, even halting operations at some clinics and hospitals. Billions of dollars in payments to providers were held up, and Change still hasn’t fully recovered.
At the hearing this week, lawmakers expressed frustration that nobody from United, which acquired Change in 2022, attended. There was talk of a possible subpoena.
Witty is expected to testify soon before the Senate Finance Committee.
The New York attorney general’s office has asked a judge to void the $175 million bond former President Trump secured to put off paying the larger monetary damage award in his civil fraud case.
State lawyers said in court filings Friday that the former president and his co-defendants — the Trump Organization and its top executives, including his two eldest sons — failed to prove the surety Trump used to obtain the bond actually has the money to back it.
They also say the defendants did not show that “sufficiently secure and ascertainable” collateral backs the bond.
“Based on the foregoing, the People respectfully request that the Court deny Movants’ motion to justify the surety, declare the Bond to be without effect and order that any replacement bond be posted within seven days, along with such other and further relief the Court deems necessary and appropriate,” lawyers with New York Attorney General Letitia James’s (D) office wrote in a 26-page filing.
Trump’s bond was secured by the California-based Knight Specialty Insurance Company.
State lawyers argued Knight is a “small insurer that is not authorized to write business in New York” and, until Trump, had “never before written a surety bond in New York.”
The company has a total policyholder surplus of just $138 million, the filing says. Under New York state law, companies like Knight can’t expose themselves to liabilities — like a bond — or any potential loss greater than 10 percent of their surplus.
“Based on KSIC’s policyholder surplus in its most recent annual financial statement of $138,441,671, the limitation of loss on any one risk that KSIC is permitted to write is $13.8 million,” the lawyers wrote. “The face amount of the bond exceeds this limitation by $161.2 million.”
The state also argued that because Trump still has access to the $175 million in cash he placed in an account as collateral, the court should find that he and his codefendants “failed to meet their burden to demonstrate that the Bond is ‘sufficiently collateralized by identifiable assets.'”
Judge Arthur Engoron ruled earlier this year that Trump, the Trump Organization and top executives conspired to alter Trump’s net worth for tax and insurance benefits. He ordered them to pay a combined $464 million, plus interest.
Trump’s bond ensures that James’s office can’t collect the multimillion-dollar judgment against the defendants while they appeal and pauses other penalties. The bond amount was originally set at the full judgment amount, but an appeals panel agreed to lower the price when Trump’s lawyers said it would be “impossible” for the former president to secure a full bond.
The judge is expected to hold a hearing Monday to discuss the issues raised by the attorney general’s office. The hearing is set to run in parallel to opening statements in Trump’s New York criminal trial.
The title of this post should have been given toa studythat was published in 2022. I have missed that publication until recently, perhaps because of its uninformative title: “Nursing home quality, COVID-19 deaths, and excess mortality.” There is nothing to suggest earthshaking findings.
The inference from the lengthy paper is the opposite of what many would have thought: the greater the mitigation efforts in US nursing homes, the higher the death toll during the pandemic. Those efforts not only largely failed to reduce Covid mortality, but they also added non-Covid deaths. The more they tried to mitigate, the worse the outcome was.
A working version of the paper was circulated in October 2020. The first manuscript was submitted to the journal in March 2021, and it took the authors ten months to submit the final version, much longer than the typical timeline. I assume that the authors did not expect the results yet courageously accepted them. To ensure their validity, they added more data and performed extraordinary “robustness analysis.” It seems that the authors worked hard to please reviewers (likely anonymous) who probably preferred that the manuscript be buried.
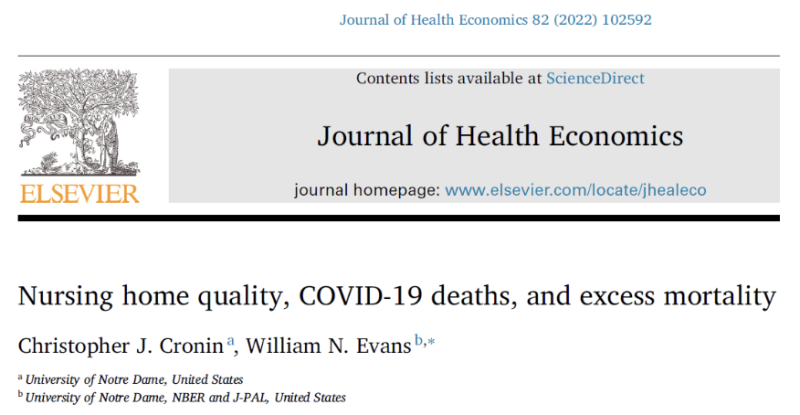
I constructed three samples of key results from Table 3, highlighted numbers, and added arrows.
Without going into a technical explanation, the highlighted numbers above tell us that overall mortality in US nursing homes was associated with their quality ranking: the higher the quality, the higher the number of deaths. These results are consistent in three consecutive periods: May through September 2020, September through December 2020, and December 2020 through April 2021. Moreover, the relationship between quality ranking and mortality became stronger over time. It is also “monotonic;” namely, observed in every consecutive pair of quality ranking. (The group of 1-star ranking is missing because it serves as the reference for others.)
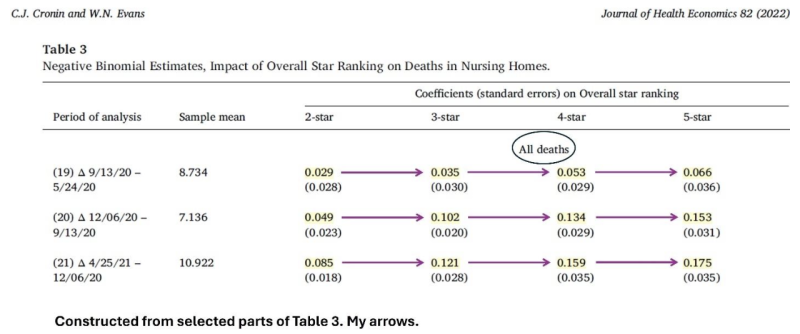
Why was the quality ranking of a nursing home related directly, rather than inversely, to all-cause mortality during the pandemic? The answer is also shown in Table 3: the higher the ranking, the higher the number of non-Covid deaths.
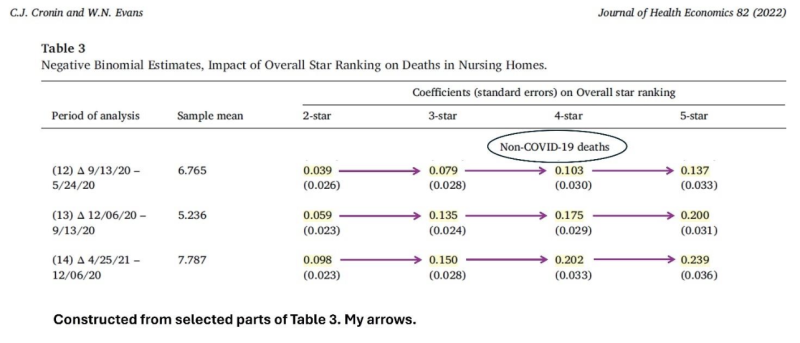
Was the quality ranking of a nursing home inversely associated with Covid mortality?
Only in the first period do we observe an inverse association (three consecutive negative numbers). And it was insufficient to negate the direct association with non-Covid mortality.
Why did non-Covid mortality increase when the quality of a nursing home was higher?
The authors propose the most likely causal explanation. Quality ranking was a surrogate for adherence to mitigation guidelines. The higher the quality of a nursing home, the more strictly official guidelines were followed. And those guidelines had a wide range of adverse consequences, which the authors describe as “unfortunate downsides to these early policies that could have negatively impacted nursing home resident health.”
Citing relevant studies, they specify some of the mechanisms: extreme isolation, which may be deadly in Alzheimer’s; unsupervised meals leading to weight loss; a lack of communal activities, which reduced exercise and increased the time spent in bed; and a large decline in regular medical care of frail, elderly residents. These plausible mechanisms are documented in horrific personal stories.
I diverge from the authors on two main points. First, they don’t say a word about the substantial misattribution of deaths to Covid. Second, and more important, they believe that the vaccination of nursing home residents played a significant role in early 2021.
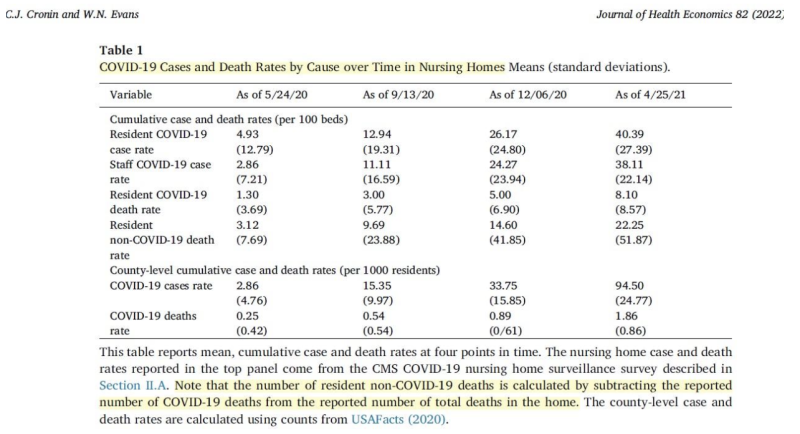
By now, it is widely acknowledged that Covid vaccines did not reduce the risk of infection, but officials still claim that they reduced the risk of death if infected. Using data from Table 1 in the article, I will show that the case fatality rate (CFR) did not decrease during the vaccination campaign. Nor did Covid vaccines reduce Covid and all-cause mortality in that vulnerable population. Lastly, I will use the paper’s data to compute rough estimates of the excess mortality in US nursing homes and the share that should be attributed to detrimental mitigation efforts.
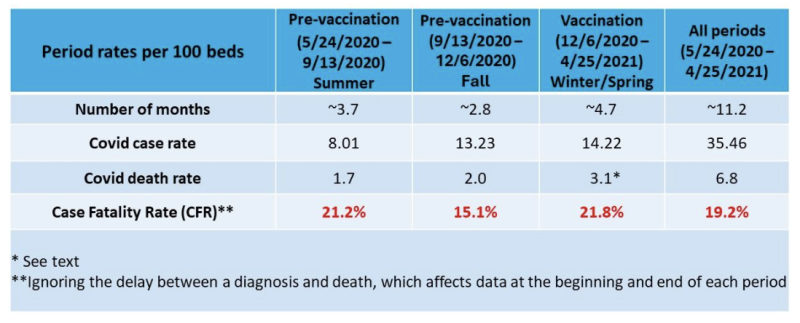
The authors reported only cumulative rates at four time points, unevenly spaced. The last period contained the vaccination campaign (as of January 2021). My table below shows the rates of Covid cases and deaths in each period and overall (almost one year).
The CFR, as computed from the paper’s data, did not decrease in the last period, despite a high rate of vaccination in nursing homes. It was virtually identical to the CFR in the first period and higher than the CFR in the second period.
Based on CDC data, about 25% of Covid deaths in the US were misattributed in the first five months of 2021. These deaths were caused by other underlying conditions and would have happened even if there were no pandemic. They did not contribute to excess mortality. If we apply the correction to the last period (winter/spring), the rate of true Covid deaths was 2.3 (instead of 3.1), and the CFR was 16.2% (2.3/14.22), similar to the CFR in the immediate pre-vaccination period.
Both computations lead to the same conclusion. The CFR during the vaccination period was similar to the CFR in an earlier period, either the first or the second.
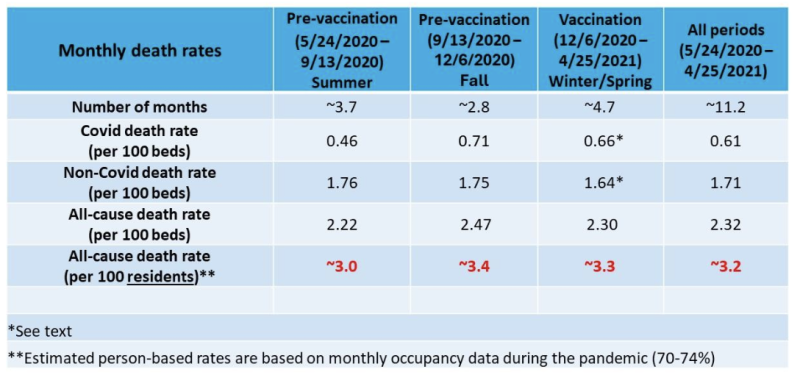
The next table shows the monthly death rates (Covid, non-Covid, and all-cause) in the same periods. These rates (per 100 beds) were computed by dividing the period rate by the number of days in the period and multiplying by 30.
In the last row, I estimated the rate of all-cause deaths per 100 residents (%) by taking into account estimates of occupancy in each period.
If we apply the previous correction to the third period (winter/spring), the rate of true Covid deaths was 0.49 instead of 0.66, and the rate of non-Covid deaths was 1.81 instead of 1.64. These rates (per 100 beds) are similar to the corresponding rates in the first period (0.46 and 1.76). They are somewhat higher when taking lower occupancy into account. Either way, the monthly rate of Covid deaths during the vaccination period was not lower than the rate in the first period without vaccines.
The interim period was the shortest. As expected every year, monthly all-cause mortality was higher in the fall than in the summer, but it appears to be due to higher Covid mortality alone. This might not be the case, though, as the misattribution of deaths to Covid likely persisted throughout the pandemic at a varying rate. Time-dependent variation in misattribution, which is difficult to estimate, adds some uncertainty to any study of trends in Covid mortality.
Regardless, all-cause mortality per 100 residents did not materially differ between winter/spring and fall (last row). Neither the benefit of Covid vaccines, if any, nor their (unquestionable) short-term fatality is reflected in all-cause mortality. The frequencies were low.
Overall, about 3.2% of the residents have died each month. That’s almost 40% in one year. Can we estimate the excess mortality in this vulnerable population?
Rough calculations below, along with heuristic arguments.
The high mortality rate of people who are admitted to a nursing home is well known, but data are sparse. A US study dating back to 2012–2013 reported 35% yearly mortality of newly admitted residents. However, residents who are observed during one year have been admitted at various earlier times. Some of them are older but perhaps healthier (survivors). A Norwegian study of newly admitted residents found stable mortality of the surviving cohort over three years of follow-up. About one-third of the remaining cohort have died each year.
If the expected (“normal”) mortality in US nursing homes was 33% during the pandemic, the excess mortality over 12 months was around 20%. And if the expected mortality was only 30%, excess mortality was around 30%.
Although the death toll was very high, many lives were probably shortened by months, not years.
How much of the excess mortality may be attributed to futile and harmful mitigation efforts, as revealed in the paper? I offer a tentative range of estimates.
Table 3 shows estimates of excess mortality in each period for a 2-star quality ranking or higher, relative to nursing homes with a 1-star ranking. Combining these numbers by simple math yields about 10% excess mortality in 2–5-star nursing homes during a period of almost one year.
If the lowest-ranking nursing homes (1-star) roughly estimate the expected mortality with no mitigation at all, the toll of mitigation efforts (10%) accounted for one-third (10/30) to half (10/20) of the excess mortality in 12 months.
Is my range of estimates plausible? Can we attribute at least one-third of the excess mortality in nursing homes to mitigation efforts? Could it have been even higher?
I think that the authors of the article would not be surprised. For example, they write (page 14):
In the latter of these three periods (row 21), five-star homes experienced 17.5 percent more total deaths than one-star homes…By our estimates, all of these excess deaths are due to non-Covid causes.
An anonymous nursing home expert, who analyzed data from the country’s 15,000 facilities, was cited back in November 2020: “…for every two COVID-19 victims in long-term care, there is another who died prematurely of other causes.” And matters got worse in that winter.
I have studied the share of non-Covid excess deaths in the US, in Arizona, in my Arizona county, and in Israel. The results have been consistent. At least 15%, and up to one-third, of the excess mortality may be attributed to the panic response in all its forms, including futile mitigation efforts. That share must have been higher in the frail population of nursing homes. It was certainly not lower.
The study I discussed here should have been featured in mainstream media. The findings are solid and devastating. I suspect that few have heard about it. That’s not surprising, however.
Dr. Eyal Shahar is a professor emeritus of public health in epidemiology and biostatistics. His research focuses on epidemiology and methodology. In recent years, Dr. Shahar has also made significant contributions to research methodology, especially in the domain of causal diagrams and biases.
The CDC finds that covid-19 vaccines are NOT linked to fatal heart problems in young men. The NBC headline is provocative, but does the study prove what is claimed?
It looked at “a total of 1,292 deaths among persons aged 16–30 years”. which occurred “In Oregon, during June 2021–December 2022, “
Here is what the paper says
“Among the 24 male decedents with an mRNA COVID-19 vaccination record in IIS, two (8%) died within 100 days of having received the vaccine...”
As a professor of epidemiology, I have no idea why the authors or CDC thinks this proves anything. The sample size is woefully inadequate to see a safety signal for cardiac death. Worse, relying on death certificates biases the whole enterprise as doctors who code death certificates may not even be aware of the potential risk and may themselves wrongly exonerate the vaccine.
At one point in the paper, the authors actually admit the truth, the “small population size made it less likely that Oregon would see a rare event such as sudden cardiac death among adolescents and young adults.”
Of course! The study has no power to find a signal for cardiac deaths. And we know for certain that men between 16 and 24 have a 1 in 3000 risk of myocarditis (from many studies) from dose 1 and roughly a 1 in 10,000 risk of myocarditis from dose 3 (KP experience). We know that sudden cardiac death or death from myocarditis will be much less frequent than this. We also know that the reduction in hospitalization from COVID19 vaccination was largest for dose 1 and unknown for dose 3, or in kids who had COVID.
With these facts, almost surely, the vaccine does increase death from cardiac reasons (as some people get myocarditis and some of these people will die), though this signal will be small, and too small to see in a single, low population state (Oregon). We also know the risk benefit balance of the vaccine may shift with repeat doses and natural immunity. This is epidemiology 101. It is a shame that the CDC is not willing to actually conduct the correct studies to quantify the risk, and continues to publish misinformation.
Vinay Prasad, Hematology OncologyMedicineHealth PolicyEpidemiology Professor
"He's the guy who went running to Adam Schiff and blew the whistle on Trump for what he thought was an improper phone call with the president of Ukraine. This first impeachment of Trump always smelled like a political op, and now after we've reviewed over 1,000 emails from former Vice President Biden's office, it now looks more like a coverup operation," Sperry said. "The sleazy business Biden was doing in Ukraine, we're talking about the extortion of [former Ukrainian president] Poroshenko to fire the prosecutor who was investigating Burisma, which was paying Biden's son millions of dollars at the time."
"In the Obama White House, Ciaramella was the NSC director over Ukraine policy, and he was attached to Vice President Biden's office because Obama had made Biden his 'point man' on Ukraine policy. He was right in the middle of all this policymaking on Ukraine, he was in the middle of talking to the Ukrainian prosecutors, bringing them into the White House, taking notes with Biden in the room, flying over to Ukraine on Air Force Two. He was also looped in on all the communications regarding controlling damage about the unseemly optics that the vice president's son was taking millions of dollars from a corrupt oligarch when Biden was giving speeches saying we need to crack down on corruption in Ukraine."
"White House communications director for Vice President Biden then, Kate Bedingfield, was cc'ing Ciaramella on all these damage control emails. He had a front-row seat to all these shenanigans Biden was doing in Ukraine regarding his son and Burisma," Sperry continued. "He was in the loop and he never disclosed this potential conflict to Adam Schiff when he filed the complaint against Donald Trump."