by 'A Midwestern Doctor' via 'The Forgotten Side Of Medicine' substack,
This excellent presentation meticulously breaks down exactly what went awry throughout COVID-19. What everyone needs to know is summarized below...
Ron Johnson has gradually become one of my favorite senators in American history. In 2020, he repeatedly advocated for early COVID-19 treatments to be made available to Americans (which had they been made available would have ended the pandemic).
Throughout 2021, he spoke out against the vaccine mandates and in November hosted a panel at the Senate which scrutinized the federal vaccine mandates and exposed how poorly those who experienced severe COVID-19 vaccine injuries were being treated. In January 2022, he hosted a panel which scrutinized the entire COVID-19 response, and in December of 2022, he hosted a panel focusing on everything we now know about the vaccines.
Being one of the most outspoken critics of the vaccination program in American history got him a lot of pushback, and in 2022, he decided to postpone his retirement to go through a grueling re-election campaign so there would be someone in the government who could advocate for everyone whose lives had been ruined by the COVID vaccines.
Despite being public enemy number one of the pharmaceutical industry, Johnson narrowly won, becoming the first politician in America’s history to run on the vaccine safety issue and win. Since then Johnson has kept his promise and fought for the vaccine injured (along with taking a variety of other difficult but important positions such as giving one of the most poignant speeches I’ve heard on the Ukraine War when he tried to block the Senate from continuing to fund it).
A lot of work has gone into producing each of the vaccine panels he’s hosted. On Monday, he hosted “Federal Health Agencies and the COVID Cartel: What Are They Hiding?” When it was all said and done, I believe this panel was the most effective presentation I have seen for explaining what happened throughout COVID-19 and waking people up to how much they have been lied to. Because of this I strongly encourage you to watch or share his presentation with people who you think might be open to understanding exactly what was done to all of us. This article will begin with his entire panel:
Note: I have been struggling to find the best term for these criminals. The four I’ve used are listed below; I would appreciate knowing what you think is the best one.
What's the best term for the COVID criminals?
The COVID Cartel
The Pandemic Profiteers
The Pandemic Industrial Complex
The Biosecurity Agenda
Lastly, for those who prefer to read, a transcript of Johnson’s symposium can be found here.
Note: for each of the videos embedded within this article, I (or the Vigilant Fox) edited them down to their most important parts. A lot of time was put into this article because of the importance of what was presented.
Federal Health Agencies and the COVID Cartel: What Are They Hiding?
Since the entire panel was 4 hours long, I recognize that many of you will not be able to watch all of it. For that reason, I tried to highlight what I felt were it’s most important parts.
First, in Johnson’s opening statement, he discusses just how hard it has been over the last three years to get any of the information his office is legally entitled to from the government. For example with (Fauci’s) NIH:
We are down to the last 50 pages [of the 4000 he originally requested]. They will not release these. It's been now going close to 2 years. This is what has been provided to us. Do you think there might be some incriminating information in this?
Likewise, these agencies have completely brushed off all evidence something is wrong. For example, with the NIH:
Just like former NIH director Francis Collins Collins told me when I asked about all the deaths being reported on VAERS, [he said], “Senator, people die.” The fact that both of these statements are as true as they are callous highlights the challenge we face in exposing the truth.
While with the FDA:
I've written 4 [letters on hot-lots] starting in December of 2021. The first letter compared 25,000 lots of COVID vaccine to 22,000 lots of flu vaccine. One COVID lot had 5,297 adverse reactions associated with it. The worst flu lot had a 137. So 5,300 versus 137.
365 COVID lots had more than 100 adverse events. Only 10 flu lots had more than 100. And 80% of the serious adverse events, those with emergency room visits, hospitalization, or death were associated with only 5% of the lots. So, again, to me, I'm from manufacturing. That shows to me a manufacturing process out of control.
[It] took us a year to get some kind of response and, basically, response from the agencies was, “we don't see any variation in lots.”
Johnson then illustrates how the current political climate has undermined everything science once stood for:
“Vaccine injuries are rare.” “The benefits outweigh the risk and that the science is clear and overwhelming.” “And anyone challenging this narrative is an is an anti science conspiracy theorist.” In other words, second opinions are not allowed. To me, this attitude is the antithesis of science.
I am amazed at the knowledge mankind has obtained over the millennia. But I would argue that what we don't know vastly exceeds what we do know. So as we pursue truth, we must pursue it with the humility that that reality demands.
Johnson’s opening statement was then followed by Robert Malone:
I'll be succinct. The SARS CoV 2 modified mRNA based vaccine products were deployed via emergency use authorization without adequate nonclinical and clinical testing and without full disclosure of known patient risk and efficacy data. This violated well established legislatively mandated patient informed consent requirements. The FDA and HHS justified these actions as necessary due to reliance on deeply flawed modeling data indicating that SARS CoV 2 was associated with an infection fatality rate of 3.4%.
Note: the IFR was subsequently shown to average between 0.018%-0.03% for everyone under 60 and was approximately 0.506% for those between 60-69 years of age.
Subsequent clinical research experience has revealed a number of problems with the genetic vaccine technology based SARS COV 2 products, which have been marketed as vaccines. In most cases, there has been an effort to obscure or deny facts in public communication by government and pharmaceutical industry representatives.
Malone then listed the key issues with the vaccines, to which Johnson replied:
Doctor Malone, I think one of the things that always bothers me is [that] so much of what we're learning in terms of harms of these vaccine was clearly known before they were rolled out.
Jessica Rose spoke next. After concisely summarizing all of the issues that had been found within VAERS, she concluded with:
Standard operating procedures for analysis of safety signals emergent from VAERS when utilized reveal causal links between the COVID 19 injectable products and the adverse events investigated. Standard operating procedures are not being followed by the owners of the data, namely CDC, HHS, and FDA, and this equates to hiding the millions of people reporting not only adverse events but injuries in the context of the COVID 19 injectable products.
Note: Rose also reviews the science behind why vaccinated individuals keep on catching COVID-19.
Edward Dowd then concisely presented the years of work his team has done to quantify just how devastating the vaccines have been for the world.
To quote part of Dowd’s testimony:
When analyzing the excess death human cost…in 2020, there were approximately 458,000 excess deaths, of which 73% were aged 65 and older and 15 to 64 comprising just 27%. However, in 2021, with the rollout of the “safe and effective vaccine,” there were approximately another 500,000 excess deaths, but a mix shift had occurred from older to younger. In 2021, the 65 plus age category was [only] 57…while the 15 to 64 cohort increased to 43%.
The absolute excess death increase from 2020 to 2021 for the productive working age 15 to 64 was 73% [124,000 to 215,000].
The total excess death since the rollout of the vaccine in the US, including 21, 22, and 23 is approximately 1,100,000. We estimate the economic cost, productive working age people dying at $15,600,000,000 When analyzing disabilities, it's interesting to note that there were no excess disabilities in 2020.
Using the civilian labor force, we have calculated an increase of 2,300,000 individuals with disabilities costing the economy an estimated $77,000,000,000. When analyzing lost work time, which we call injuries, we estimate 28,400,000 individuals are chronically absent resulting in an estimated economic cost of a $135,000,000,000 since 2021…Obviously, the policy cure was undeniably worse than the illness.
Kevin McKernan then discussed his groundbreaking discovery that there was widespread DNA plasmid contamination of the COVID vaccines and how horrendously the drug regulators have responded to that discovery.
This work has been replicated by many labs around the world, and now the FDA, the EMA, and even Health Canada, have admitted to this. The regulatory agents have admitted that Pfizer also omitted the SV40 sequences that are in their vaccine. They've deemed this contamination to be of little consequence, claiming the DNA is of too little concentration to matter or to be containing DNA of no functional consequence. These statements are false and are not supported by any independent testing by these regulators.
After the regulators have admitted to being deceived, they asked the opinion of the party that deceived them how bad was the deception. They shockingly believe the answer they were given, which is that these sequences have no relevance to plasmid manufacturing. As someone who has worked on the Human Genome Project manufacturing millions of plasmids, I can assure you that this is an overt lie. DNA contamination can lead to insertional mutagenesis. This is actually declared in Moderna's own patent regarding the mRNA vaccines.
This is also supported by Lim et al, which speaks to the rate of spontaneous integration in the genome during transfection. We are using transfection after all with LMPs. The SV40 DNA is in fact functional. It is published as a potent gene therapy tool in a nuclear targeting sequence as described by David Dean et al.
The SV40 promoter DNA is also known to bind to the tumor suppressor gene known as p53.
Note: p53 defects are commonly linked to cancers.
We've applied these vaccine system cancer cell lines and have evidence that it enters the cell and can survive several cell divisions. We have preliminary evidence, although this requires replication in other labs, that this DNA can integrate into the genome. We found 2 spike sequence integration events in ovarian cancer cell lines of CAR 3 into chromosome 12 and 19 very recently. Since these vaccines were expected to only contain mRNA, they were never assessed for genotoxicity studies. These studies were therefore being conducted as guinea pig US citizens as we witnessed an unprecedented rise in cancer drug sales since the vaccines rolled out.
It is time for our representatives to repeal or review the PDUFA Act of 1992. This act allows regulators to defray the cost of regulation by accepting payments directly from the companies they regulate. Over half of the FDA's budget is sourced through this act.
Note: I discussed the significance of the vaccine plasmid contamination in more detail here.
Dr. David Gortler (who previously served as a senior advisor at the FDA) then explains why the contamination and widespread variability we are seeing in the vaccines (e.g., the hot lots) being completely ignored is so unprecedented:
Federal rules requiring ingredient transparency date all the way back, believe it or not, to 1862 [and] it's the whole reason the FDA was started in 1906. Prior to COVIDsRNA injections, the FDA had approved 4 different RNA based products. Onpattro, shown here, was the 1st RNA product approved back in 2018…as you can see by looking at this label, Onpattro prominently details the exact structure, milligram strength, and molecular weight. Highlighted in green at the very top, you'll see it specifies [what its] lipid nanoparticles are engineered for.
In contrast to the previous labels I've shown, here is the official FDA label for COVID RNA injections. As you can see just looking at it, it details a lot less information. We don't [even] have the structure.
Of note, in pharmacology, even very minor deviations in any molecular structure can mean the difference between a drug and a poison…The lack of transparency means that scientists can't use modeling to test lipid nanoparticles for safety receptor specificity or analyze inequality [in batches of those products].
Unfortunately, around 70% of the 127 page document that explains the methodology to perform quality control on RNA injections are redacted much like the document I've shown here.
Next Dr. Harvey Risch discusses the “crushingly obsessive push to COVID vaccinate every living person on the planet” and provides a concise overview of the horrific bioweapons industry which gave birth to COVID-19 and then tried to pivot to vaccinating everyone rather than accept responsibility for what it had done.
Note: This catastrophic industry is discussed in more detail here (e.g., I highlighted how numerous modern diseases are the results of lab leaks).
Next, Barbara Loe Fisher, an activist who has spent decades fighting for vaccine safety shared the broader context of what we are now dealing with.
I worked with parents in congress to secure safety and informed consent provisions in the National Childhood Vaccine Injury Act of 1986. It was an historic law, the first official acknowledgment by government that federally licensed and state mandated vaccines can and do injure and kill some children. In January, my eyewitness perspective of how and why child vaccine victims and their parents were betrayed after that law was passed 38 years ago, was featured in a 2 hour conversation I had on the Highwire.
I encourage everyone to watch it and learn how parents trusted that the 5 years of work we put into that 1986 act to successfully secure life saving, informing, recording, reporting, and research provisions in it, and to protect the legal right of vaccine victims to sue vaccine manufacturers for product design defects, and to sue negligent doctors for medical malpractice, and to create an expedited, more just, less traumatic federal vaccine injury compensation system alternative to a lawsuit were all destroyed by congressional amendments, by federal health agencies, and the US Supreme Court after that law was passed. Following that betrayal of trust, Congress directed federal agencies to create lucrative public private business partnerships with the pharmaceutical industry, a business deal that has broken America's public health system.
Note: I previously wrote about how the 1986 Vaccine Injury Act forced the government to create VAERS (as parents had no way to report vaccine injuries) and ever since that time, the government has done everything it could to undermine VAERS.
Johnson then shares a poignant observation with Fisher that illustrates how effectively the pharmaceutical industry has bought out our media:
By the way,I became aware of you from that excellent documentary which I would also recommend. What struck me about [it] is back then in 1982 through 1986, you could talk about these things. You could advocate for your child who's vaccine injured. You weren't ostracized. You were actually welcomed here in the senate by people like Senator Hatch and Senator Kennedy and you got this [law] signed by Ronald Reagan.
To which Fisher replies:
I never imagined when I began this work in 1982 that the day would come when I would not be able to exercise freedom of thought and conscience in the country I love. And I thank you for allowing me to exercise that right today.
Next, Bryan Hooker, the parent of a severely vaccine injured adult son shares his 23 years of work (e.g., 15 peer-reviewed papers) to get the data on vaccine injury the CDC has been hiding for decades.
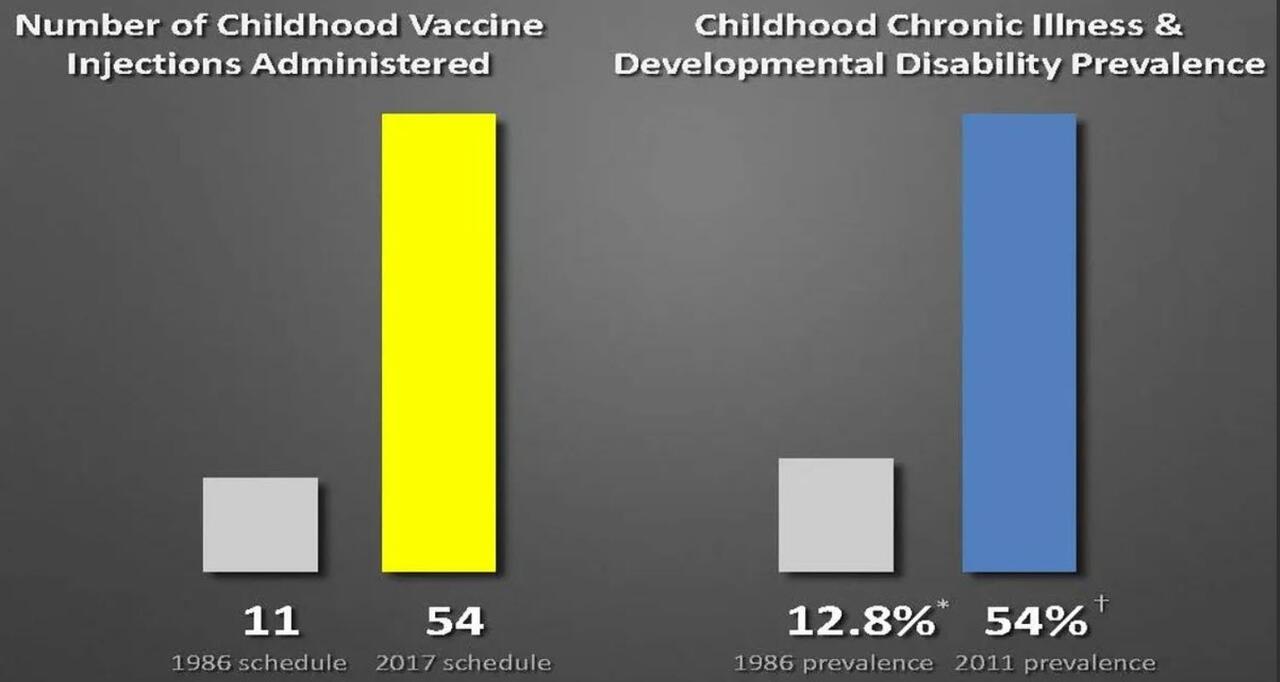
In 1962, children received 5 vaccine doses, and in 1986, the schedule expanded to 25 doses of 5 different vaccine formulations. Shortly after the passage of the 1986 National Childhood Vaccine Injury Act, the law was amended to essentially erect a liability shield protecting vaccine manufacturers, and the schedule expanded dramatically. By 2023, 73 doses of 16 different vaccine formulations were given to children up to age 18. [As we discovered through lawsuits] the FDA approved these formulations individually only with minimal and inadequate safety testing, and the CDC has never tested the cumulative effect of the vaccine schedule on childhood health outcomes.
Since [proper trials] are really the only way to establish that a pharmaceutical product is safe, it is misinformation to state that the vaccines are safe.
However, independent researchers have assessed the outcomes of vaccinated versus unvaccinated children.
This [study] demonstrates that vaccinated children were at least twice as likely to be diagnosed with developmental delays, ear infections, and gastrointestinal disorders.
[In this study] a control group of over 1800 unvaccinated children recruited from 46 different states in the US were compared to the national average rates of the listed disorders…For each of the autoimmune, neurodevelopmental, and other disorders considered, the unvaccinated group fares much better with incidence rates between 4-20 times lower than their vaccinated counterparts.
The CDC has a database called the vaccine safety data link. It's over 10,000,000 individuals with 2,000,000 children from 10 participating HMOs. I would say that within that database, there were at least 10,000 unvaccinated children that can be studied.
Neither do they they publish the results [discovered from that data], nor do they let any independent scientist in to look at that information. [That’s] because [they know] the bloated vaccination schedule is responsible is in part responsible for the epidemic of chronic disorders that we see in children in the United States.
Note: Hooker also discusses the evidence the COVID-19 vaccine harms children (e.g., that it appears to kill 30 children for each child it saves from COVID and has given many of our children myocarditis).
Next, Del Bigtree discusses the decade of work he and the non-profit ICAN have conducted to get that data from the government:
In his talk, he puts the results of a recent study which monitored 99 million people for 45 days post vaccination into context. It found that their risk for a variety of severe conditions increased by 2-7 times, something which quickly adds up as you when consider how many of those “rare” conditions exist (that often take more than 45 days to appear) and how many vaccines they’ve received. These results is turn sheds a light on exactly what’s been happening to our children.
Every one of the childhood vaccines has a similar [lengthy] list of [severe] side effects. Though they are considered rare, how rare is it when you multiply roughly 50 potential side effects 72 times, which is the total number of doses given to a child by the time they're 18. The revelations from the recent study of the COVID vaccine explains what we have been saying for years. Vaccines are not completely safe, and [though] those side effects are rare. What happens when you add them altogether?
Bigtree then shows this slide (which references this study and this study):
Next, Dr. Sabine Hazan shared how her [self-funded] research to evaluate the use of existing therapies to treat COVID-19 was blocked by the FDA, her discovery that the severity of COVID-19 was directly linked to a loss of bifidobacteria in the gut and that the vaccine also caused a loss of bifidobacteria in the gut. She then contrasted this to how previous research she did (which supported the pharmaceutical industry) never ran into similar road blocks.
Note: I synopsized that research here.
Pierre Kory then discussed the lengthy number of mechanisms which are in place to ensure that repurposed (off-patent) drugs can never have enough evidence to be acknowledged as treatments for a disease someone is profiting off of.
Note: this talk has already been seen by over 1.6 million people on Twitter.
Next, Christian Perron MD PhD (former chairman of the WHO’s committee on vaccines and communicable diseases) recounted how early in the pandemic, he completed a study which showed hydroxychloroquine and azithromycin dramatically lowered the death rate from COVID-19. A political backlash forced the withdraw of his study and he was fired from his 26 year professorship.
Before long France then banned the use of hydroxychloroquine and began enacting harsher and harsher sanctions against French dissidents like Perron who tried to tell the truth—eventually forcing Perron to publish in a French newspaper which had originally been created to defy the Nazis (as every other publication censored him).
Perron was followed by Raphael Lataster PhD, who is one of the leading researchers working with the BMJ (one of the top 5 medical journals) to expose the fraud within the COVID vaccine trials:
These [abhorrent] policies [e.g., the vaccine mandates] were justified via claims about the vaccine’s effectiveness and safety. Now recent research published in major medical journals reveals that these claims were highly exaggerated…we have found in the studies varying definitions of fully vaccinated and unvaccinated. And, generally, what we find with the term fully vaccinated is that they are ignoring COVID cases, COVID infections, in the partially vaccinated…that effect was found to be up to 48% using data from Pfizer's trial as an example.
We can't be sure what the actual exaggeration is because we aren't supplied with all the data. So it's impossible to actually know. But it looks like there are huge exaggerations of effectiveness because of what you could call manipulation of the data. So if these [omitted COVID cases] were included, or if even just some of these were included, we could have an effectiveness of the vaccines of around 10%...[which]is well below the 50% required for approval. Furthermore, looking to safety in the clinical trials, adverse effect counting windows are again incredibly short.
Note: Lataster also discusses many of the safety issues with the vaccines that were demonstrated within the trial data but hidden from the public (e.g., that the vaccines have a significant risk of myocarditis) and states “now Pfizer also admits that they're still trying, this is a quote ‘to determine if Cominati is safe and effective and if there is a myocarditispericarditis association that should be noted’. That's on clinicaltrials.gov still right now. They're trying to find out if it's safe and effective right now.”
Award winning investigative journalist Lara Logan then provides a poignant summary of how her profession has been hijacked by the government and how a variety of shadowy organizations now enforce this vast propaganda apparatus. This was the most compelling part of her talk:
Note: Her testimony was followed by one from Jason Christoff, a propaganda expert, who explained why flooding the population with a single narrative and way of thinking has caused many people to adopt completely dysfunctional beliefs at odds with everything they’d held dear
They were then followed by Rodney Palmer, who was a Canadian journalist for 20 years, sharing his perspectives on the current state of the media.
If the news reporters did their jobs instead of reporting propaganda, this fraud would have been exposed from the outset.
Censorship is what actually caused these deaths. It was the lie that assured us it was safe when it wasn't, and it still isn't
In America, it's much worse. The vaccine companies are allowed to sponsor the news directly…To a visiting Canadian, the news here looks like one big ad for pharmaceutical products. It's a bit of a culture shock when you turn on the TV. There wouldn't even be a US newscast without Pharma ads. So the reporters on your newscasts are all conflicted.
They can't bite the hand that feeds them. They can't possibly investigate the most important stories of our time.
It appears that the reporters are actually colluding with their sponsors to break FDA advertising laws. FDA law requires them to conspicuously describe the known risks of any pharmaceutical product [which news anchors promoting vaccines never do.
The good news is no one believes the TV news anymore. Only 15% of Canadians, 15%, are getting the boosters.
[The media has] now canceled lunchtime news hours. It's canceled weekend newscasts. After these reporters are laid off, we'll only be left with the trusted favor of the trusted faces of our favorite news anchors, delivering the propaganda of the day, instead of the news of the day. But when those trusted faces are telling us lies, they're like a super weapon aimed directly at us. The news anchors are now the finger on the trigger in that game of Russian roulette.
When the news is poisoned, so is Democracy…most every other country is letting this happen, but where goes America, so goes the world. You have a unique role in setting the moral tone for Western democracies.
So I respectfully recommend that the senate investigate the role of American television news networks, including with pharmaceutical advertisers to skirt the FDA laws that require them to declare the known risks of a pharmaceutical product. This investigation should extend to any reporters, news anchors, editors, and executives who lied to their audience about the safety of the COVID vaccines.
Note: Palmer also describes how he gradually saw the corrupting influence of the pharmaceutical industry enter Canada’s media over the last decade. One of the most compelling observations he shared was that during the pandemic, the doctors who spoke on television didn’t talk like doctors but instead appeared to have corporate media training, which he took as an early sign a lengthy PR campaign was being enacted to sell as many vaccines as possible.
Next, Matthias Desmet provided a concise summary of the crowd psychology which explained how it was possible for so many people to refuse to see what was being hidden from them, even thing after thing happened which made it clear we were all being lied to:
Note: I recently completed an article relating Desmet’s work on crowd psychology to how individuals commonly become trapped in cults and dangerous spiritual practices.
Brett Weinstein then describes the institutional breakdown gripping our society and the malicious forces which are taking away each thing we had previously depended upon for truth and justice (e.g., our premier scientific apparatus). I wanted to quote one exchange he had with Johnson:
[Johnson] Now I kind of want to ask you, I describe my eyes being opened up, certainly during COVID to a number of things…Can you just describe your [red pill] journey here?
[Weinstein] Well, I think we are all on a similar journey. I did not think that I was naive 7 years ago, and then I learned that I had been very naive and I keep learning that lesson. Each new discovery reveals that I was missing something that was right in front of me, and I think that's actually the hallmark of the exact pattern I'm describing.
Canadian Randy Hillier served in Ontario’s parliament for 15 years and was the first member to publicly oppose his government's response to COVID. Like Canada’s citizens, Hillier was targeted by the government for doing so, and argues we are at the tip of a slippery slope with this. In this part of his testimony, he shares how Ontario’s leadership told him they made the decision to continually coverup the damage of the COVID policies because they felt the political consequences would be too severe if they admitted their mistakes:
Next, Dr. Sorin Titus Muncaciu shared his experience as a Romanian member of parliament who watched the central authorities use every tool at their disposal to forcefully vaccinate Romania.
We are a party having probably 10% of the votes we got in the parliament in 2020, and we, from the very beginning of this pandemic, we decided that the rights of the people to decide if they accept, or [do not accept receiving] an experimental drug should be respected.
When the European Union started behaving like the USSR with those commissars coming to us and mister Barnier came to Romania. This gentleman was the commissioner for internal affairs of the European Union and pushed us, pushed the Romanian parliament to vote [for COVID vaccine mandates].
But in Romania the problem they face is that we are 40 years after a communist dictatorship, 30, 34 years after a communist dictatorship. And it's in our genes to distrust the government because we knew every time a communist government is saying anything or is directing anything, we knew that's a lie, that's something that we should not trust or we should not follow.
We did everything in the book that we could to stop that and we stopped it. And, as a consequence to that, the Romanian rate of vaccination was probably less than half of what the other European countries experienced or United States, Canada and Australia [experienced]. And, therefore we can compare now the low rate and the excess mortality. And that's the best proof I can bring to the table is the fact that having a relationship between a low rate of vaccination and low excess mortality, which is right there you see it on the, Romania is the last country on the right which means we have negative excess mortality while all the other countries in Europe have positive excess mortality.
Rob Roos (a European member of Parliament) and Phillip Kruse (a lawyer) then discussed who actually funds the WHO and the disastrous treaty it is trying to sneak through which will force everyone to comply with the pandemic cartel and silence anyone who challenges their next pandemic response.
Note: I discussed this treaty and the grass roots effort to stop it in more detail here. I consider that article to be one of the most important articles I’ve published on Substack.
Finally, Ryan Cole concluded the talk by discussing how he was punished for speaking out, how everything which happened throughout the pandemic has violated our fundamental constitutional rights and how critical it is for us to reclaim what our Founding Fathers fought for.
Note: for anyone considering being a whistleblower, Johnson requested for you to contact his office here.
Conclusion
Since Johnson packed this presentation with so many impactful points, it was quite hard to decide which was the best one to conclude it with. Eventually however, I settled on this one, which while brief, I believe is the critically important message all Americans can agree with:
It is remarkable how much each successive panel Johnson has hosted has improved upon the one which preceded it. I consider this to be both a product of how dedicated each participant has been to fixing this mess and how much the alternative media has facilitated the production of high quality information that has rapidly unravelled the immensely complex web we were trapped within.
Without each of your supporting the wonderful community of dissident authors on Substack, much of this would likely have never happened, and I thank each of you from the bottom of my heart for giving me the opportunity to be part of it.
Lastly, if you have anyone close to you who is on the fence about the vaccines, please consider sharing this article or a video of Johnson’s panel with them; it’s something than can persuade people who are at last beginning to become open to hearing the truth and we have reached the moment where it is critical for the truth to reach as many people as possible.
https://www.zerohedge.com/covid-19/sen-johnsons-senate-panel-vaccines-red-pill-weve-all-been-waiting
