Four years have passed since the onset of COVID-19 and the global mishandling of its spread. Now, the same governments and international organizations that lied about the last pandemic are negotiating a new pandemic agreement and amendments to the International Health Regulations (IHR) at the World Health Organization (WHO).
The main culprit hasn’t changed. Although the Chinese Communist Party (CCP) has never been held accountable for its complete refusal to adhere to previous IHR agreements or its ongoing obstruction of a thorough investigation into the virus’s origins, Beijing is now collaborating with the Biden administration on this new accord.
So naturally, the new agreement advances China’s interests. Successive drafts focus on everything, from sending taxpayer dollars overseas to weakening intellectual property rights and empowering the WHO over the national sovereignty of the United States. Yes, that’s the same WHO that failed to insert a team of global experts in the first few weeks of the COVID-19 outbreak in China (as required by IHR), instead capitulating to the CCP and allowing it to define the international response.
The latest version of the agreement even mandates that parties provide financial and technical assistance to developing countries. Of course, the United States has a long, robust history of providing such assistance—President George W. Bush’s President’s Emergency Plan for AIDS Relief (PEPFAR) is one good example—but such assistance has always been voluntary, not obligatory.
Unsurprisingly, China stands to benefit from these provisions intended to help “poor” countries. Despite having the second-largest economy in the world, the United Nations considers China to be a “developing country.” That’s right. The country that started the COVID-19 pandemic will not only suffer zero consequences for its actions but, should the United States sign this agreement, stand to benefit from mandatory transfers of funds from U.S. taxpayers.
China would also benefit from other provisions in the agreement that push governments to promote “sustainable and geographically diversified production” of pandemic-related products (like vaccines), invest in developing country capacity and access to proprietary research, use the “flexibilities” of the Agreement on Trade-Related Aspects of Intellectual Property Rights to override patents, and encourage rights holders to forego or reduce royalties and consider time-bound waivers of intellectual property rights.
China, notorious for its theft of intellectual property, would be sure to exploit this privilege.
All this would severely curtail future investment in health research—exactly the opposite incentive that should be applied if we are to be prepared for a future pandemic. And to make matters worse, the agreement almost entirely ignores addressing the countless shortcomings of current international processes in responding to pandemics, such as obligating governments to grant immediate access to international health expert teams to assess the threat of suspected outbreaks and to provide full and timely disclosure of genomic data.
Of course, overseeing sustainable and geographically diversified production, massive transfers, and distribution of up to 20 percent of diagnostics, therapeutics, or vaccines during a pandemic comes with a hefty price tag. The exact amount is not specified, but it is sure to include several commas.
In addition, the agreement would take a sledgehammer to American First Amendment free speech rights. The willingness of governments to use the pandemic to clamp down on unpopular ideas and opinions to “protect” public health and safety has proven durable. And this new agreement instructs governments to “cooperate, in accordance with national law, in preventing misinformation and disinformation.” China and Russia need no encouragement to censor speech. However, such language in an international agreement will encourage those in free countries who similarly wish to suppress unpopular opinions under the guise of countering misinformation and disinformation.
Indeed, the WHO itself seems offended by criticism. Earlier this year, Director-General Tedros Adhanom Ghebreyesus said that negotiations were occurring in a very difficult environment, facing a “torrent of fake news, lies, and conspiracy theories.” Ironically, this argument was the same one used against conservatives who subscribed to the increasingly credible lab leak theory.
In short, the new pandemic agreement should alarm all Americans. It is far more focused on redistributing income, transferring technology, and weakening intellectual property than on preventing, detecting, and responding to pandemics in the first place. It failed to address the elephant in the room—the total lack of enforcement in the IHR—and as written, it is nothing short of a power grab by the CCP-controlled WHO.
Drug shortages in the U.S. are at an all-time high, according to the latest statistics from the American Society of Health-System Pharmacists. Thedatareveals active and ongoing shortages stand at 323 drugs as of the end of the first quarter of 2024, the highest number since the organization began tracking such information in 2001.
The American Society of Health-System Pharmacists (ASHP) reported both basic and life-saving products are on the list, including chemotherapy, pain and sedation medications and ADHD medicines. Exploding interest in GLP-1 injectables for weight loss and diabetes has also caused widespread shortages as supply simply cannot keep up with demand.
The drug classes ASHP’s data shows the highest shortages between 2019 and 2023 were antibiotics, chemo, central nervous system and hormone therapies.
According to the ASHP, 60% of the shortages were for unknown reasons, or the manufacturer would not provide an explanation. However, supply and demand, manufacturing and business decisions were split statistically in the low-percentage teens for reasons for shortages provided by drug manufacturers. Only 2% of shortages were reported due to raw material issues.
In February 2024, the U.S. Government Accountability Office (GAO) issued a report pointing to continued challenges for the FDA in the wake of the COVID-19 pandemic and staff vacancies. While the office acknowledged the FDA is working to address these issues, the report also stated, “GAO has had long-standing concerns about FDA’s ability to oversee the increasingly global drug supply chain.”
The GAO stated in its report that of the over 4,800 manufacturers providing drugs for Americans, 58% of them were overseas as of 2022. In November 2023, an Intas Pharmaceuticals plant in India was flagged by the agency for a number of quality issues. Import of its chemo drug, cisplatin, and others manufactured there have been halted to the U.S. by the FDA.
Multiple doses of Eli Lilly’s Mounjaro, its diabetes-indicated GLP-1, will be in short supply through April 2024. This was not a surprise as the World Health Organization previously issued a warning about GLP-1 shortages in January 2024. Lilly’s current shortage impacts the higher dose strengths. Its competitor Novo Nordisk has also struggled with shortages due to high demand since Wegovy was approved by the FDA.
The U.S. Department of Justice announced Wednesday it hasfiled a False Claims Act complaintagainstRegeneron Pharmaceuticals, alleging that the company “fraudulently inflated Medicare reimbursement rates” for its eye therapy Eylea (aflibercept).
In its 49-page complaint, the Department of Justice (DOJ) claimed that Regeneron knowingly provided the Centers for Medicare and Medicaid Services with false average sales price reports, which omitted price concessions associated with credit card processing fees.
“Regeneron knew that paying the credit card processing fees enabled customers to purchase Eylea from distributors with a credit card at a lower amount than the distributors otherwise would have charged,” the DOJ wrote in its complaint, adding that by using credit cards, the pharma’s clients—which included retina and ophthalmic clinics—would also be entitled to other benefits, such as cash-back rewards.
These benefits translated to “hundreds of thousands, and in some cases millions, of dollars in ‘cash back’” from Eylea purchases, the DOJ alleged. In some cases, these Eylea cash-back rewards “went directly into doctors’ pockets,” according to the complaint, with some physicians even using their personal credit cards to purchase Eylea.
Regeneron “deliberately chose not to report” these credit card benefits as price concessions, which in turn inflated Medicare’s reimbursement rates for Eylea, according to the DOJ.
“Falsely reported average sales prices cost the Medicare system hundreds of millions of dollars and we will make every effort to prevent such practices,” Joshua Levy, acting U.S. Attorney for the District of Massachusetts, said in a statement.
If found guilty, Regeneron will be on the hook for up to three times the amount of its losses, plus other applicable penalties.
"Regeneron believes that the allegations against us are without merit. The complaint, which follows a Civil Investigative Demand from the U.S. Department of Justice in June 2021, and which the Company previously disclosed, relates to the Company’s lawful reimbursement of costs incurred by our specialty distributors," a company spokesperson told BioSpace in an emailed statement.
"The Government’s complaint demonstrates a fundamental misunderstanding of drug price reporting standards. Regeneron has fully cooperated with the Government’s investigation and will vigorously defend itself in court," the spokesperson said.
Eylea is a recombinant fusion protein that works by blocking both the vascular endothelial growth factor-A and the placental growth factor, both of which play a crucial role in the formation of new blood vessels.
The drug first won the FDA’s approval in 2011 for the treatment of neovascular age-related macular degeneration and has since picked up several other indications, including diabetic macular edema, diabetic retinopathy and macular edema after retinal vein occlusion.
The U.S. Cybersecurity and Infrastructure Security Agency said Russian government-backed hackers have used their access to Microsoft's email system to steal correspondence between officials and the tech giant, an emergency directive by the U.S. watchdog released on Thursday showed.
In the directive dated April 2, the agency warned that hackers were exploiting authentication details shared by email to try to break into Microsoft's customer systems, including those of an unspecified number of government agencies.
The warning that government agencies are being targeted using stolen Microsoft emails follows the company's announcement in March that it was still wrestling with the intruders, which it nicknames "Midnight Blizzard."
That disclosure, which set alarm bells ringing across the cybersecurity industry, was followed just last week by a report from the U.S. Cyber Safety Review Board which said that a separate hack - blamed on China - had been preventable, faulting the company for cybersecurity lapses and a deliberate lack of transparency.
CISA declined to name agencies that might have been affected. Microsoft said in an email that it was "working with our customers to help them investigate and mitigate. This includes working with CISA on an emergency directive to provide guidance to government agencies."
The Russian Embassy in Washington, which in the past has denied being behind hacking campaigns, did not immediately return a message seeking comment.
CISA warned that the hackers might have gone after non-governmental groups as well.
"Other organizations may also have been impacted by the exfiltration of Microsoft corporate email," CISA said, encouraging customers to contact Microsoft for further details.
Nat gas prices at the Waha hub in the Permian basin in Texas slumped to a negative price of -$2.00 per million British thermal units (MMBtu) this week as the recent rise in oil prices prompts producers to bring drilled but uncompleted wells online,OilPricereported.
As the U.S. benchmark oil price, West Texas Intermediate, hit $85 per barrel—the highest level in nearly six months, Texas producers keep pumping crude, but their wells also produce gas, which basically has nowhere to go.
While producers are chasing higher realizations for the crude they pump, they are depressing further an already depressed U.S. natural gas market, which has been oversupplied for months due to a milder winter and lower demand for heating and electricity.
Producers in West Texas are hit by the negative price of natural gas at the Waha hub, which means that they have to pay for someone to take that gas. But demand just isn’t there.
“They’re bringing these drilled, uncompleted wells online because the price of oil is higher,” Dennis Kissler, senior vice president for trading at BOK Financial Securities, told Bloomberg.
“It’s flooding the market with gas, and you’ve got no demand,” Kissler added.
Yet, signs have started to emerge that the natural gas glut may have started to hold back drilling in parts of the Permian basin.
U.S. oil producers are not in a rush to significantly boost crude production despite oil prices hovering at a six-month high, as multi-year low natural gas prices and higher costs are weighing on the industry, analysts and executives told Reuters earlier this month.
Oil producers in America are also mindful of the investor demands for higher returns, not necessarily higher production.
“Natural gas is currently pricing at or below costs of production,” an executive at an exploration and production company said in comments in the latest quarterly Dallas Fed Energy Survey released at the end of March.
Back in late 2022, when "Western democracies" bombastically unveiled theatrical sanctions against Putin, capping the price at which imports of Russian oil were permitted to no higher than $60, we said that this was one of the biggest farces in modern history, not only because it was an optical play that was made entirely for public consumption (as nobody in the west actually wanted to curtail Russian oil exports as the outcome would be a devastating surge of inflation asBiden now realizes), but also because there was no enforcement mechanism to cap the price at $60 and no more.
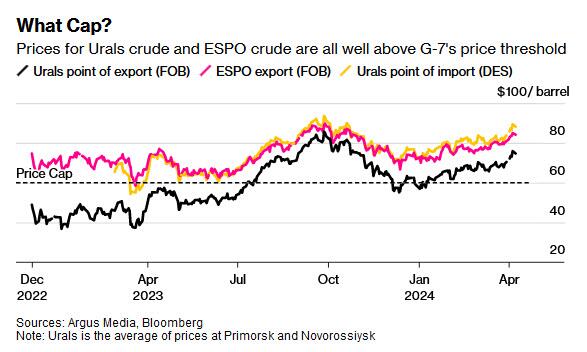
We were right, again, and today Bloomberg reports that "Russian oil is trading far in excess of a Group of Seven price cap that’s supposed to deprive Moscow of revenue for its war in Ukraine, suggesting significant non-compliance with the measure", which anyone with half a working brain would have expected to happen, which of course excludes virtually all "democratic" bureaucrats who implemented this idiotic sanction (which only ended up making the Vitol oil traders billionaires).
According to data from Argus Media, whose price assessments are followed by some G-7 nations involved in the cap, Russian flagship Urals grade oil is now selling for $75 a barrel at the point it leaves ports in the Baltic Sea and Black Sea. A Treasury official told Bloomberg that US officials are tracking the price increase, which they attribute to broader geopolitical dynamics, as the alternative - admitting they are idiots, would be a bit too introspective.
As a reminder, the Russian embaro cap requires that any western company involved in transporting Russian oil receives a so-called attestation, a document vouching that the cargo cost $60-a barrel or less. If it doesn’t, they’re not allowed to provide their services. The fact that Argus’s prices are so far above that level creates what Bloomberg called a "dissonance", but what we would call, a giant slap on the face of the Biden administration which nobody takes seriously any more.
While Urals has been above $60 almost all year, this month’s surge to well above $70 will stretch the credibility of those attestations for traders wanting to keep using western services. Not like anyone actually thought those attestations had any credibility to begin with since the governments enforcing them were so clearly interested in having everyone ignore them.
Bloomberg data showed that in March, 23% of the nation’s crude oil shipments had insurance against spills and collisions provided by members of the International Group of P&I Clubs. That means traders would have vouched that the cargoes cost well below where Argus assessed the Urals price to be, which was clearly not the case, and means that at least a quarter of Russian oil shippers are fabricating data. A smaller proportion moved on Greek tankers, all of which had cover from IG clubs, also requiring attestation.
Hilariously, the idiots in the Biden admin told Bloomberg that the cap is still having its intended effect, reducing the amount of money the Kremlin receives from oil sales by forcing the commodity to either be sold under the cap via western services, or through Russia’s shadow fleet. Which, of course, is absolutely not the case and Putin is currently rolling in the cash from selling oil to the same European nations that are supplying Ukraine with their most modern weapons which Putin then handily blows up and reverse engineers. The US plans to continue the enforcement of the cap by sanctioning vessels operating in the shadow fleet, but will not do so in response to any specific market moves, the official said, requesting anonymity to discuss internal deliberations, and for the reason that it would be extremely embarrassing if his name were to become public.
A European Commission spokesperson said the bloc is aware of the risk of the price cap being dodged, and is committed to steps that deprive Russia of revenue while simultaneously “supporting global energy market stability.” It’s also constantly reviewing existing measures to enforce the cap and prevent its violation or circumvention, the spokesperson said, adding that such measures require unanimity among member states. In other words, Europe knew from day one that the Russian oil embargo was not going to work, and now, a year and a half later, is blame the lack of "unity" for this farce.
The bloc’s most recent sanctions package was aimed at tighten the cap’s enforcement, the spokesperson said; clearly the package did not achieve the "desired outcome."
Of course, it's not just Russia that is rolling in dough: by the time Urals cargoes get to India, the grade is trading at $88 a barrel — just $3.80 below than the global benchmark for physical cargoes, Dated Brent, Argus data show. When the nation’s ESPO crude leaves the port of Kozmino in eastern Russia, it is at $84 a barrel. It hasn’t been close to the price cap for about a year.
Bloomberg concludes that since last October, "the US Treasury has shown it’s prepared to punish companies for breaches of the price cap that happened in the past" however, given its desire to avoid any actions that disrupt the flow of crude — and risk higher prices — the rally in headline Brent futures to around $90 a barrel may temper any push to do so at this time.
The use of ivermectin to treat COVID-19 is an ongoing debate. The central conflict is that while many doctors have reported success in using ivermectin, some studies published in major journals suggest it is in fact ineffective.
Even as the FDA recently has been removing misinformation it posted about ivermectin, the agency has maintained its original position regarding its effectiveness, namely that there isn’t evidence.
People who trust ivermectin claim the studies showing ineffectiveness are fraudulent, while people who are skeptical of its use for treating COVID-19 view it as an anti-science conspiracy theory.
As a professional with decades of research experience conducting dozens of clinical trials on antiviral drugs, I decided to dive deep into the studies purporting ivermectin’s ineffectiveness. What I found shocked me.
Legacy Media Report Ineffectiveness
Numerous preclinical studies have found that ivermectin has a broad range of effects on COVID-19, spanning from its initial impact on viral infection to the pathological changes the virus causes in our bodies.
Ivermectin inhibits the entire life cycle of SARS-CoV-2 in our cells from attachment, spreading, and replication (1, 2, 3).
Ivermectin exceeds the approved antiviral effects of other medications, including Paxlovid, molnupiravir and remdesivir, which only target the virus and lack anti-inflammatory and organ-protective effects. Monoclonal antibodies have to be constructed specific to each variant and are very expensive.
In the pharmaceutical industry, clinical trials are commonly used to evaluate the efficacy and safety of drugs once their mechanism is demonstrated. There are two types of clinical trials: observational and interventional.
Observational studies are often conducted by doctors in clinical, hospital, or community settings to analyze the effects of drugs. The data is collected as observed in clinical practice with minimal interference.
Many doctors have observed the positive effects of ivermectin on their patients. An observational study conducted in Brazil with over 88,000 patients showed that ivermectin reduced the rates of infection, mortality, and hospitalization by 49 percent, 92 percent, and 100 percent, respectively, compared to nonusers.
Pharmaceutical companies are required to conduct interventional studies that meet the approval standards set by the U.S. Food and Drug Administration (FDA). Randomized clinical trials (RCTs) are frequently utilized to fulfill these requirements. This type of study is considered the gold standard and involves randomly assigning one group of patients to receive a specific drug while the other group does not receive it, then comparing the outcomes.
Legally and medically, ivermectin can be prescribed off-label to treat COVID-19 since it has already been approved by the FDA for other diseases.
Although many doctors have observed the positive effects of ivermectin in treating their patients, the media has specifically highlighted data from a few selected RCTs that have concluded it is ineffective in treating COVID-19.
However, some critical aspects were overlooked in those RCTs.
Improper Dosing
A drug’s therapeutic effects can only be observed when it reaches the appropriate concentration in the body and remains there for a few days, allowing sufficient time to work.
Improper dosing was a major issue in the RCTs that found ivermectin ineffective.
Recommended Dosage
According to Merck’s package insert for ivermectin (brand name Stromectol), a single oral dose of 0.2 mg/kg was officially recommended for treating parasitic diseases. There is no official dose for COVID-19.
The recommended dosage of ivermectin for treating COVID-19 is based on the clinical experiences of physicians worldwide.
The Front Line COVID-19 Critical Care Alliance (FLCCC) guidelines recommend taking 0.4 mg/kg of ivermectin daily, immediately after exposure. Once a cumulative dose in excess of 200 mg is reached, the risk of acquiring COVID-19 has been shown to be nearly zero.
It is common for a drug with multiple indications to have different doses for different diseases.
Moreover, ivermectin should be given with food, as it has a 2.6-fold higher bioavailability when taken with food rather than on an empty stomach. The Merck package insert (revised May 2022) also supports this and states: “Administration of 30 mg ivermectin following a high-fat meal resulted in an approximate 2.5-fold increase in bioavailability relative to administration of 30 mg ivermectin in the fasted state.”
FLCCC guidelines also recommend taking ivermectin “with or just following a meal for greater absorption.”
Yet this important dosing information is not reflected in the commonly used drug prescribing resource known as the Prescribers’ Digital Reference or PDR which states: “Take the number of tablets your doctor has prescribed all at the same time with water on an empty stomach. Do not eat any food within two hours before or after taking the tablets.”
So if a person takes the dose while fasting, they are getting only 40 percent of the recommended dose. For patients with a higher body weight, the effects of underdosing could be even more significant.
RCT Studies Used Inappropriate Dosing
In the most recent PRINCIPLE trial published in March, ivermectin was used at 0.3 mg/kg for only three days. Moreover, it was designed to dose the ivermectin without food: “Participants were advised not to eat two hours before or after taking ivermectin.”
In another RCT ACTIV-6 published in JAMA in October 2022, ivermectin was dosed in a fasting status, as the protocol stated: “Ivermectin should be taken on an empty stomach with water (30 minutes before a meal or 2 hours after a meal).”
Ivermectin was reported as dosed at 0.4 mg/kg for three days—a much shorter time period than it should be. However, in the protocol Table 4 in Appendix 16.3.3, the precise dosing was as low as 0.269 mg/kg, and 0.4 mg/kg is actually only the upper dose limit—not the real dose.
According to the worldwide recognized study guideline ICH Good Clinical Practice, clinical trials must adhere to ethical principles. Failure to do so would be considered study misconduct or fraud and would violate the principle of integrity.
Another JAMA study published in March 2021 repeated the same mistake in mild COVID-19 patients by suggesting they take 0.3 mg/kg for five days on an empty stomach.
An RCT study known as TOGETHER, published in March 2022 in the New England Journal of Medicine, underdosed ivermectin with 0.4 mg/kg for only three days and did not mention dosing with food.
Nevertheless, even at this low dose, the ivermectin still reduced hospitalization rates, death, and the need for mechanical ventilation compared to a placebo.
Clinical Improvement Despite Underdosing
It is inappropriate to conclude that ivermectin was ineffective based on these RCT studies with major design flaws.
Despite the poor study design, ivermectin showed clinical benefits and saved lives.
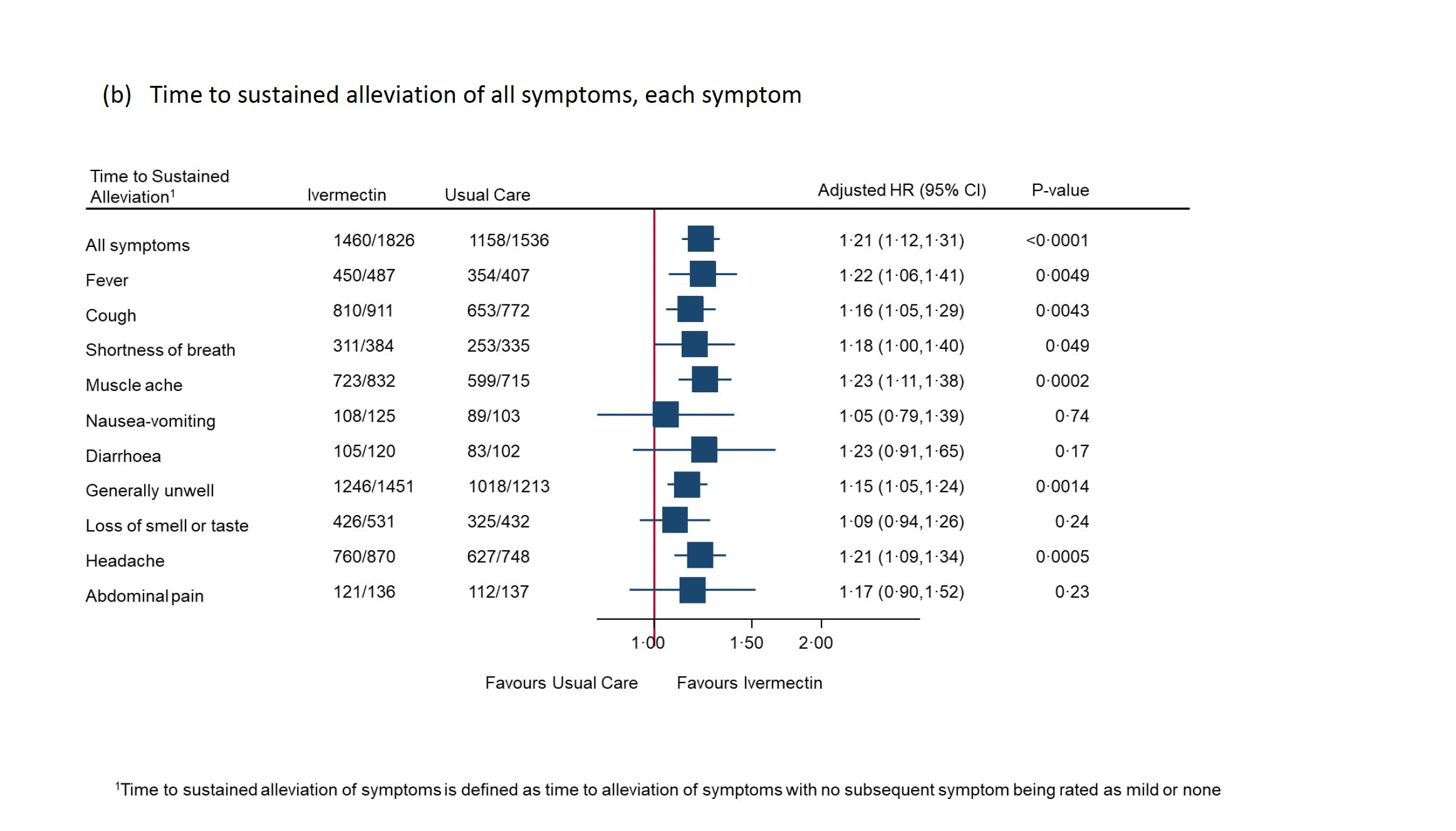
In the PRINCIPLE study, self-reported recovery was shorter in the ivermectin group than usual care, with a median decrease of 2.06 days. The statistical analysis showed that it met the predefined superiority criteria.
Furthermore, the analysis showed that ivermectin effectively reduced COVID-19-related hospitalizations and deaths. Only 1.6 percent of 2,157 patients in the ivermectin group experienced hospitalizations or deaths, compared to 4.4 percent of 3,256 patients in the usual care group.
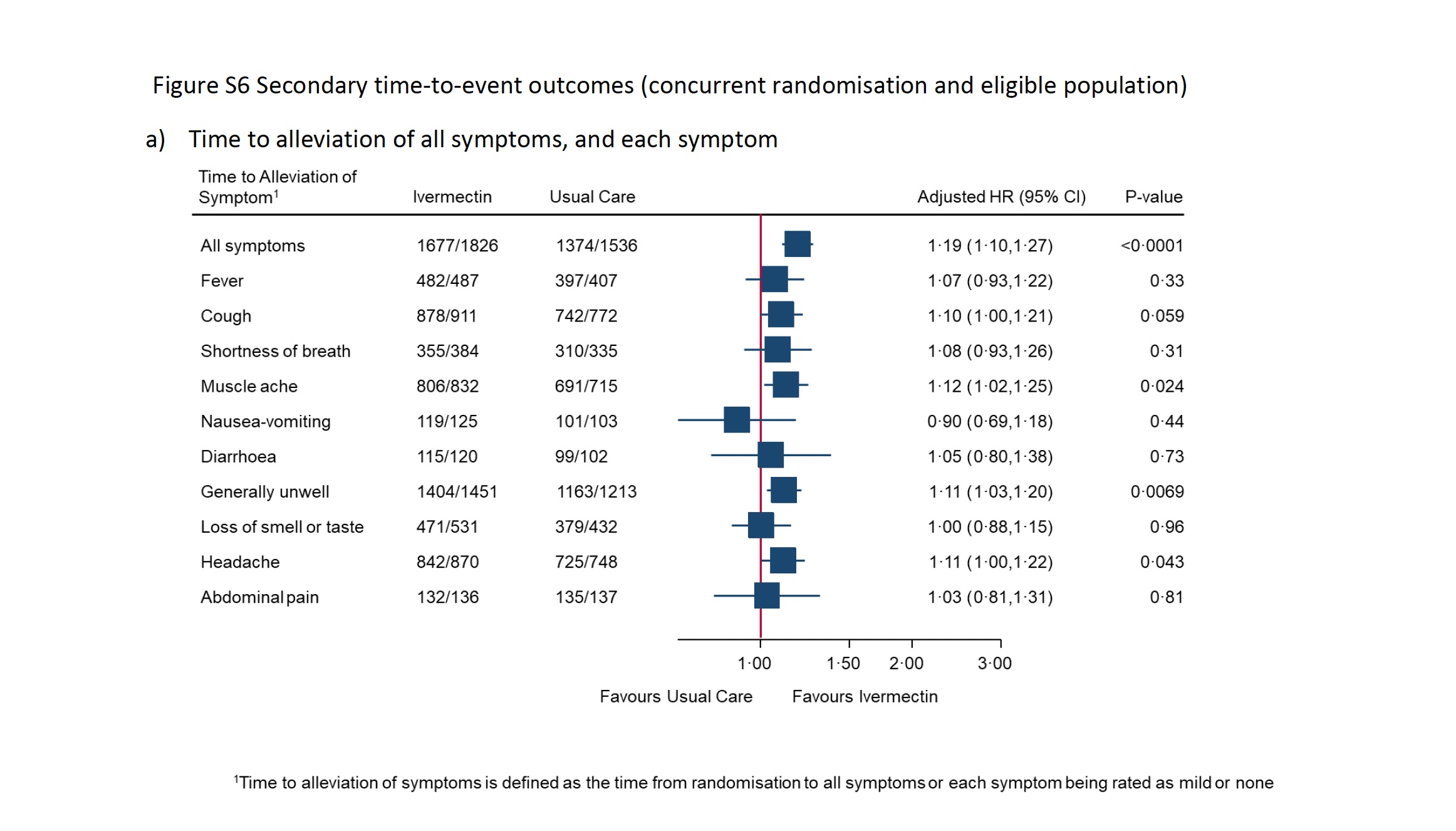
Even a low dose of ivermectin has demonstrated the potential to save lives. However, the authors concluded, “Ivermectin for COVID-19 is unlikely to provide clinically meaningful improvement in recovery, hospital admissions, or longer-term outcomes.”
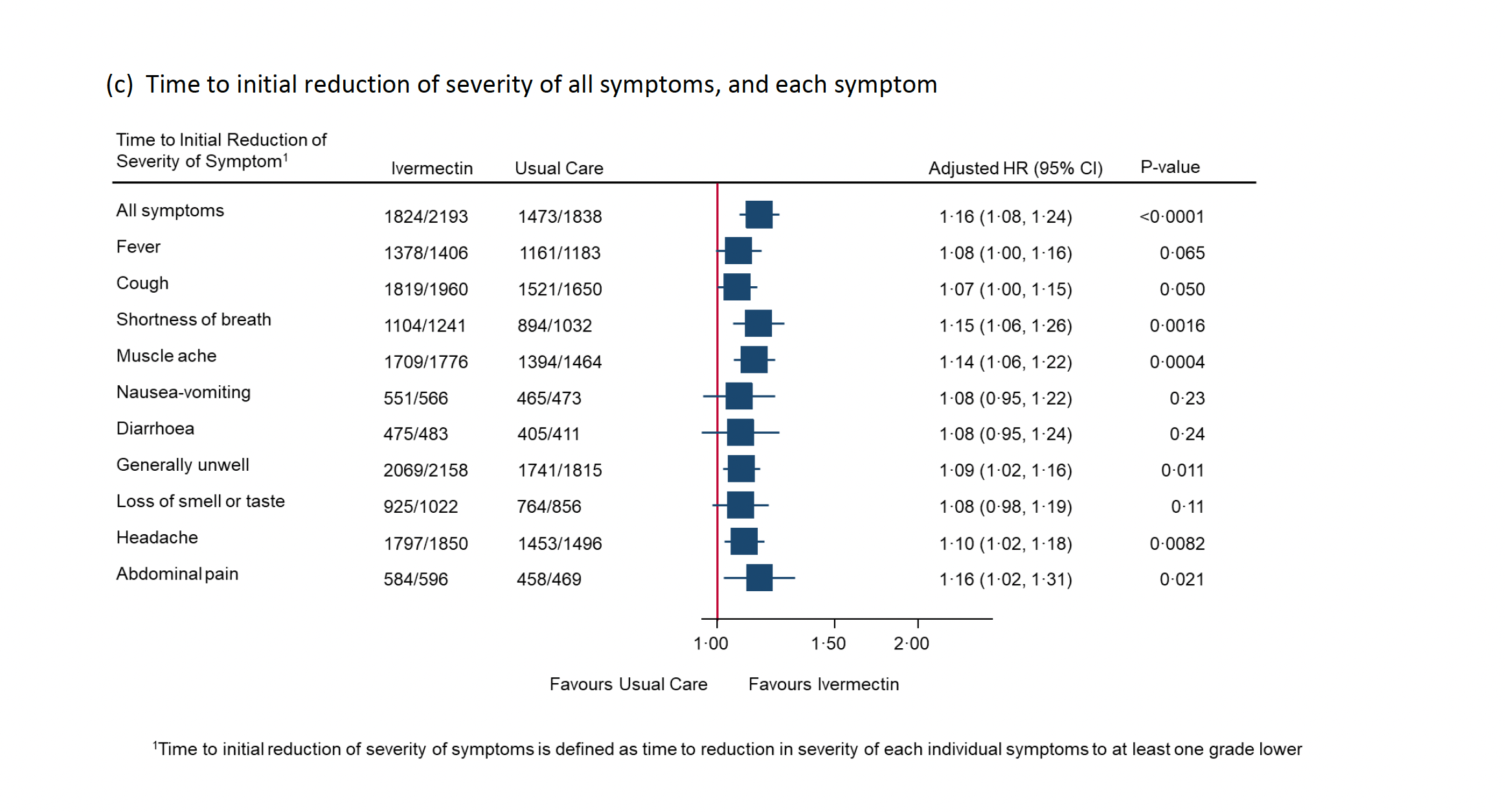
Meanwhile, the report’s appendix includes dozens of recorded clinical benefits in patients treated with ivermectin, such as the time it took to alleviate all symptoms, general unwellness, muscle aches, and headaches. The improvement of symptoms was also sustained, and the severity was reduced. Surprisingly, the source PDF was removed from the website during the writing of this article.
There are additional examples. Although the previously mentioned 2021 JAMA study underdosed patients, treatment with ivermectin reduced recovery time by two days. In the ACTIV-6 study, only one venous blood clot event was reported in 817 ivermectin-treated patients, compared to five events in 774 placebo-treated patients.
Statistical Failures
It is important to note that the definition of treatment effects in an RCT can differ from those discussed in real-life observational studies.
Sometimes, even if the results of a clinical trial demonstrate a clear effect, the conclusion may still be interpreted as ineffective due to the statistical definition of effectiveness.
Interpreting statistics can be challenging as they usually involve complicated mathematical models and numerical data that can be manipulated to support a specific agenda. Nevertheless, for the purpose of this discussion, let’s presume that all research is carried out conscientiously and without manipulative intent.
In a randomized, double-blind, placebo-controlled clinical trial with mild to moderate COVID-19 patients, none of the 55 patients in the ivermectin group died, whereas four of 57 in the placebo group died. This resulted in a comparison of zero percent versus 7 percent. Moreover, only 1.8 percent of ivermectin-treated patients needed invasive ventilation compared to 8.8 percent in the placebo group.
In other words, ivermectin reduced the risk of death by 100 percent and the need for ventilators by 80 percent.
However, the article did not provide the p-value (probability value) for the death rate comparison or the invasive ventilation of 0.102 (Table 2), which is higher than the 0.05 threshold considered to be a significant statistical difference.
P-values are commonly used to test and measure a “null hypothesis,” which states that no differences exist in the effects being studied between two groups. A finding is considered statistically significant and warrants publication when the p-value is 0.05 or less.
The p-values in this study were deemed insignificant because they were more than 0.05. Accordingly, the authors wrote that this difference was statistically insignificant and concluded that ivermectin “had shown only marginal benefit.”
How could a 100 percent reduction in death or an 80 percent reduction in ventilation be interpreted as “marginal” effects?
In the I-TECH study published in JAMA Internal Medicine in 2022, the patients treated with ivermectin had a lower mortality rate of 1.2 percent compared to 4 percent in the comparator group.
The same conclusion was made as the previous study because the p-value was 0.09 and higher than 0.05.
If the 7 million patients reported to have died from COVID-19 had been treated with ivermectin, an estimated 4.9 million lives could potentially have been saved based on the 70 percent reduced mortality rate from the I-TECH study; or 4.5 million lives could have been saved based on the 64 percent reduction of mortality in the PRINCIPLE study.
The life-saving potential of ivermectin has been hindered by the unnecessary statistical threshold. The problem of statistical significance is widespread and frequently causes confusion among scientists.
A 2016 Nature article raised concerns about the misuse of p-values. A 2019 comment in the same journal stated that “The misuse of statistical significance has done much harm to the scientific community and those who rely on scientific advice.”
The authors called for abandoning the use of statistical significance to draw conclusions regarding the effectiveness of drugs, such as stating that “drug Y does not work,” and cautioned that such conclusions may result in the dismissal of potentially life-saving drugs.
The authors also wrote: “Let’s be clear about what must stop; we should never conclude there is ‘no difference’ or ‘no association’ just because a P value is larger than a threshold such as 0.o5.”
Selection Bias
Many people, including physicians, may not be aware that interventional studies, particularly RCTs, are are prone to numerous biases, with selection bias being one of the most significant. Excluding potentially eligible individuals due to their anticipated group allocation can lead to selection bias.
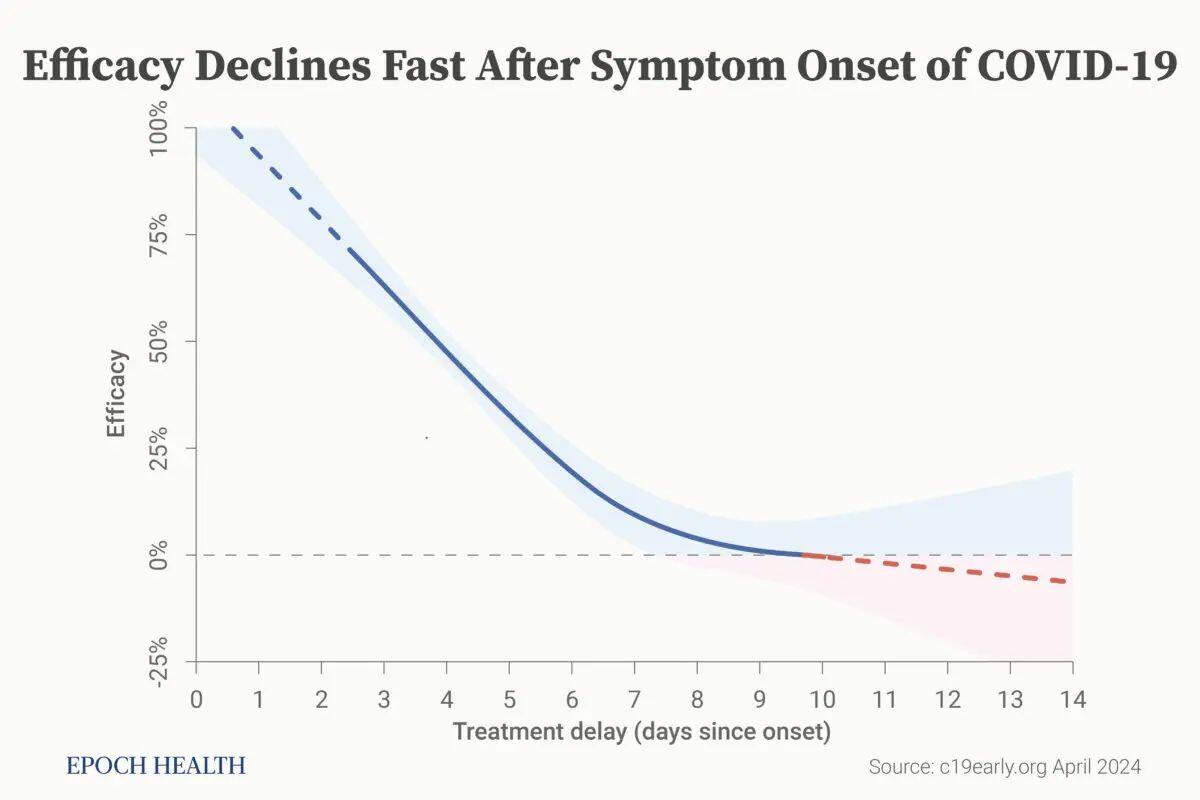
It’s common knowledge that early treatment of COVID-19 is crucial for effective results. The earlier the treatment starts, the more effective it is. These approved antivirals for COVID-19 are used shortly after COVID-19 infection and usually within a few days after symptom onset.
For example, Paxlovid and molnupiravir registration trials treated patients within only three to five days of symptom onset.
Early treatment is critical for COVID-19. Efficacy declines rapidly with treatment delay. (c19early.com)
However, in the PRINCIPLE trial, ivermectin was used for patients within 14 days of symptom onset, while ACTIV-6 treated patients an average of six days after infection.
Patients with severe kidney disease are normally excluded from phase 3 studies, as they are less likely to respond to antiviral treatment. This approach has been taken by remdesivir (protocol), molnupiravir (protocol), and Paxlovid (protocol). However, such standard exclusion criteria were not taken by the ACTIV-6 or PRINCIPLE study protocols.
Why was ivermectin treated so unfairly in these clinical trials?
It is well known that when an RCT is sponsored by Big Pharma, there is often a financial conflict of interest, as the research institutions are usually hired or funded by the pharmaceutical company. In a world where wealth often competes with ethics, how many can resist financial temptation and stay true to moral principles?
“Hidden agenda bias” occurs when a trial is conducted to demonstrate a desired outcome, rather than to answer a question. In other words, “Don’t do a trial if it won’t show you what you want to find.”
Proven Without a Profit Motive
Conducting an RCT to get a drug approved by the FDA requires money. Every drug must be managed by a professional team composed of doctors, database managers, and assistants. Professionals must secure funding, recruit a lead investigator, and find hospitals to conduct the study. An operational team must perform the study, analyze the data, and gain FDA approval.
Since ivermectin is a generic drug that lacks profitable marketing and a pharmaceutical sponsor, it’s challenging to organize and systematically manage its new application with health authorities, data, and customers.
Nevertheless, doctors worldwide have been using ivermectin to help patients and have collected valuable data.
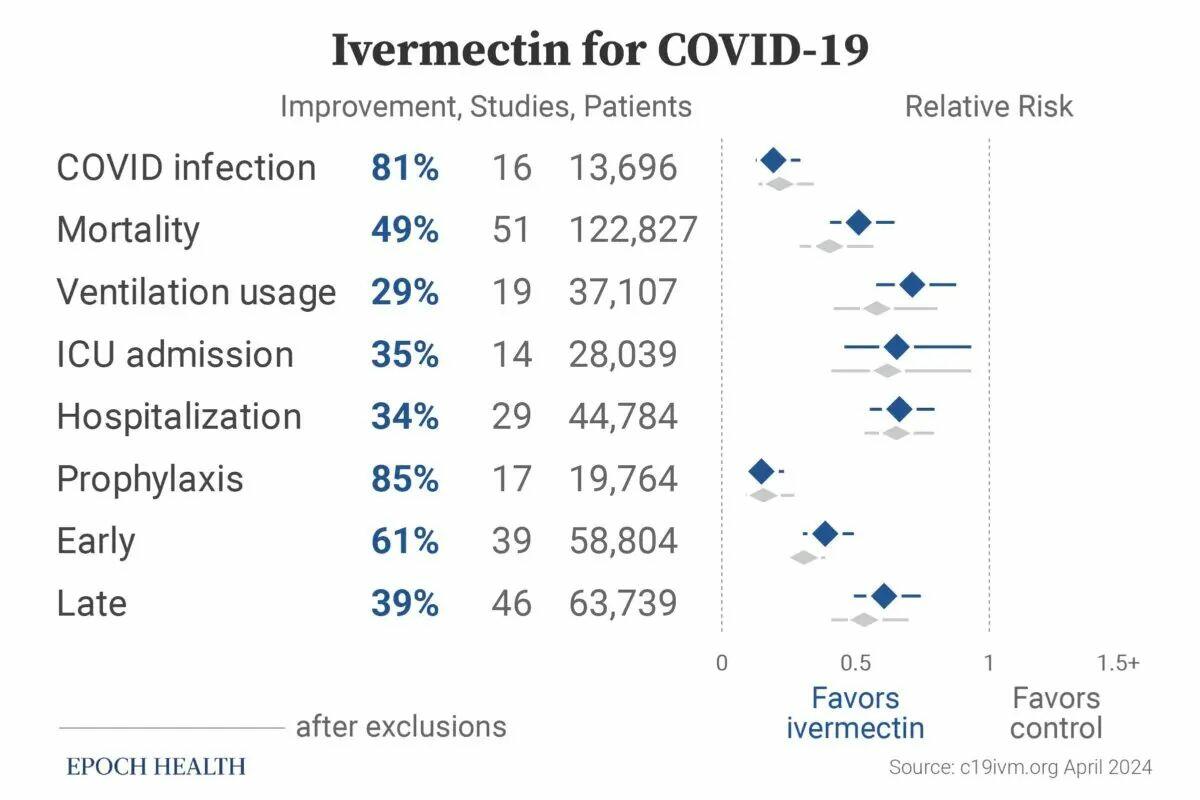
The website c19ivm.org has compiled data on 102 clinical trials proving ivermectin’s consistent effectiveness in treating COVID-19. Studies with negative conclusions about ivermectin are also included, such as the the four RCTs with recognized design flaws.
Since the beginning of the analysis, ivermectin has consistently shown efficacy. This meta-analysis provides a thorough and transparent real-time analysis of all eligible ivermectin studies.
The trials were conducted by 1,139 doctors or scientists from 29 countries with 142,307 patients. Out of the total studies, 86 have been peer-reviewed with 128,787 patients, and 49 were randomized controlled trials with 16,847 patients.
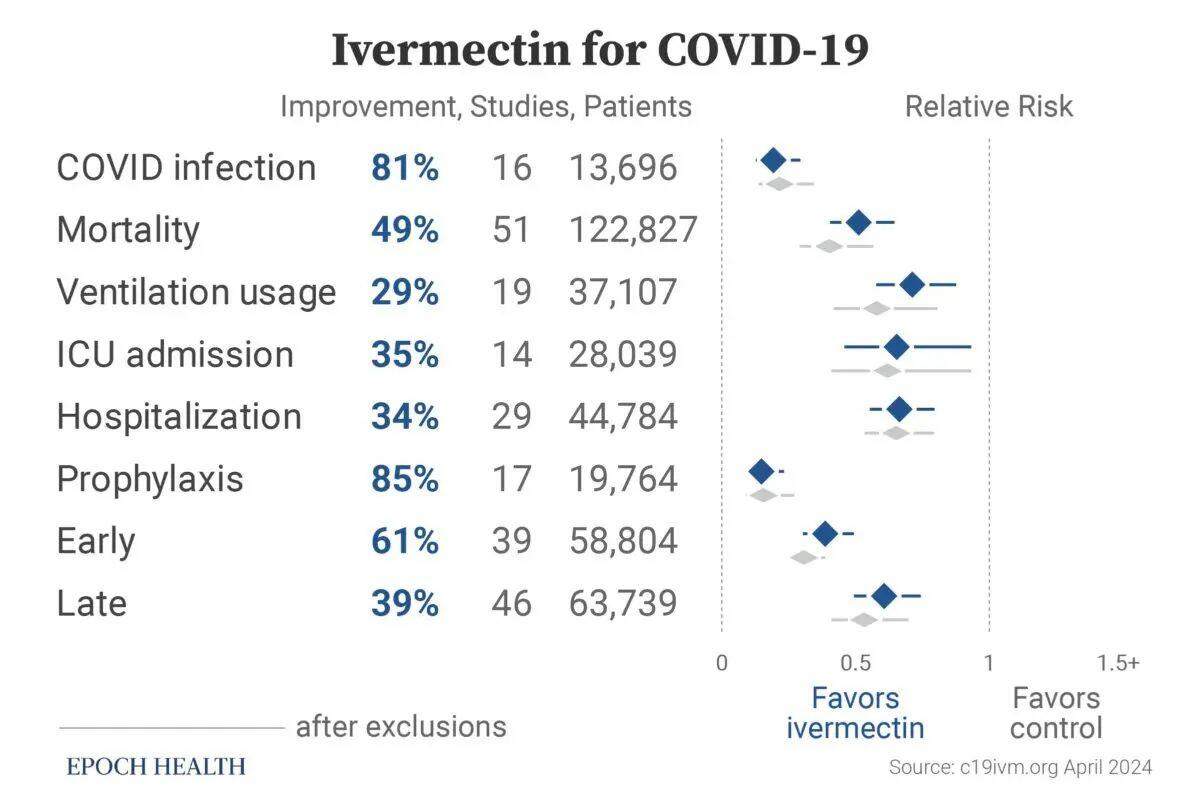
In the studies with comparative groups, ivermectin was shown to reduce the risk of COVID-19 infection by 81 percent, mortality by 49 percent, ICU admission by 35 percent, ventilation usage by 29 percent, and hospitalization by 34 percent.
In comparison to the control groups, the use of ivermectin as a preventive measure before infection reduced the most severe clinical outcomes of COVID-19 by 85 percent. When used in the early stage of COVID-19, ivermectin decreased the severity of the disease by 62 percent, and when used in late stages, it reduced the clinical severity by 39 percent. Clinical severity is measured by death, ventilation, disease progression, or hospitalization.
Ivermectin treatment effects in COVID-19 patients, based on a meta-analysis of 102 clinical trials. (c19ivm.org)
Considering the Entire Picture
It’s difficult to believe that the designers of these studies were unaware of the dosing of ivermectin. Despite all of the above analyses, the reasoning behind the ivermectin underdosing or unfavorable study design may be linked to factors beyond science.
A new drug or vaccine cannot achieve an Emergency Use Authorization (EUA) status if there is an existing viable therapeutic available. This fact alone may have impacted many decisions.
The NIH website lists only those RCTs that I found to have design flaws (or potential fraud) to justify its recommendation against the use of ivermectin in the treatment of COVID-19.
Peer-reviewed studies showing the efficacy of ivermectin in treating COVID-19 have been retracted without explanation, and doctors have been demonized,censored, and doxxed for speaking the truth.
Legacy media, including The New York Times and CNN, reported incomplete and improperly interpreted trials that failed to present an accurate representation of ivermectin’s effects.
It’s important to keep an open mind and consider the entire picture when examining the ivermectin issue, rather than dismissing it as conspiracy or misinformation. This can lead to more informed decisions that could ultimately save lives.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}