US National Security Advisor Jake Sullivan has said that authorization for Ukrainian use of American weapons for cross-border attacksextends not just to the Kharkiv region,but into other Russian regions as well, further escalating Biden's initial greenlight for such offensive operations.
Blinken in a Monday PBS interview told NewsHour's Nick Schifrin "This is not about geography, it's about common sense" and expanded the parameters for using NATO-supplied missiles. Watch the exchange below:
Jake Sullivan says US authorization for Ukrainian cross-border attacks extends not just to the Kharkiv region, but other Russian regions as well. "This is not about geography, it's about common sense" he says. Expect the parameters of this bold new policy to continue to grow pic.twitter.com/01OISmVwm3
The following is what was said in this opening section of the interview:
Schifrin: Does the agreement that you have made with Ukraine to allow Ukraine to fire American weapons just over the border into Russia at Russian forces that are about to attack into Ukraine, does that extend beyond the Kharkiv region, including into the Sumy region, where Russian forces have also been targeting Ukraine?
Sullivan: It extends to anywhere that Russian forces are coming across the border from the Russian side to the Ukrainian side to try to take additional Ukrainian territory.
Schifrin: So, that could include the Sumy region?
Sullivan: That's happened in Kharkiv.
We have seen initial indications that Russia has made exploratory moves across in Sumy. And so it would apply there as well. This is not about geography. It's about common sense. If Russia is attacking or about to attack from its territory into Ukraine, it only makes sense to allow Ukraine to hit back against the forces that are hitting it from across the border.
That's when the interviewer pointed out the obvious--that this policy will lead to open-ended and uncontrollable escalation given it takes away all parameters. "Of course, Russia is attacking Ukraine from all parts of Russia. Why draw the line there?" Schifrin asked.
Sullivan at this point essentially gave Kiev the greenlight to attack a much more expanded area inside Russia. "Well, first, we are permitting Ukrainian forces to attack Russian forces using Russia as a sanctuary in the areas where on the battlefield they are attacking from inside Russia with artillery, with other ground-based munitions," Biden's top security official said.
And what's more is that when asked about F-16s, Sullivan affirmed that Ukraine can use the US-made jets to attack Russia. Sullivan explained:
"...we have made clear — and we have seen over the course of the past two years Ukraine do this — that they can use air defense systems, including those supplied by the United States, to take Russian planes out of the sky, even if those Russian planes are in Russian airspace, if they're about to fire into Ukrainian airspace."
President Putin in late March had addressed this possibility. He said that Russian forces would then have to right to attack any airbase from which these F-16s are flown, including if they take off from within Western countries or NATO bases.
Commenting on the fresh and escalatory Sullivan remarks, independent journalist Michael Tracey said to "Expect the parameters of this bold new policy to continue to grow."
Welcome toImpact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of "improving consistency, documentation and treatment." Good news, right? Here's the definition: "Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems."
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you've had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it's long COVID. They don't even specify that it has to be a new symptom.
I'm not saying that long COVID doesn't exist. I'm not saying it isn't weird or that it can't present in diverse ways. But a case definition like this hinders our ability to figure out exactly what is going on and to identify good treatments. It mixes people with real long COVID with a ton of other people, diluting our power to do science on the condition. And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that 1 out of every 5 people have long COVID.
We are talking about this study, "Epidemiologic Features of Recovery From SARS-CoV-2 Infection," appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: "Do you think that you have had COVID-19?" and "Would you say that you are completely recovered now?" Those who said they weren't fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals' perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
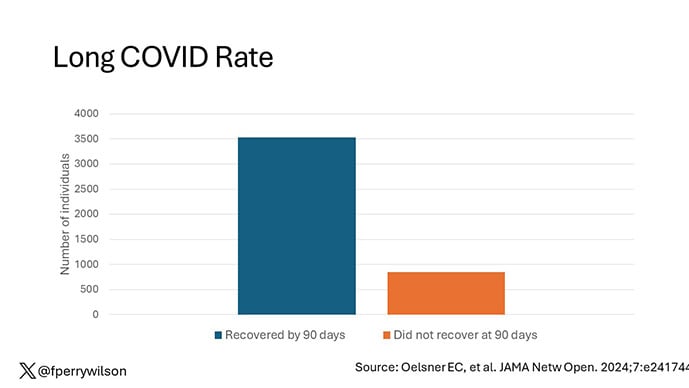
But let's look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
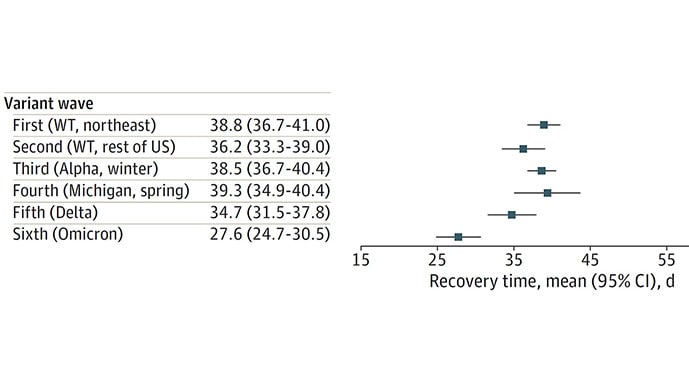
And there are some interesting trends here.
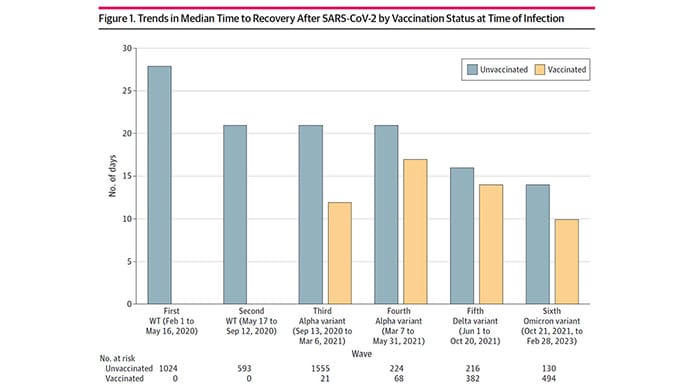
Recovery time was longer in the first waves of COVID than in the Omicron wave.
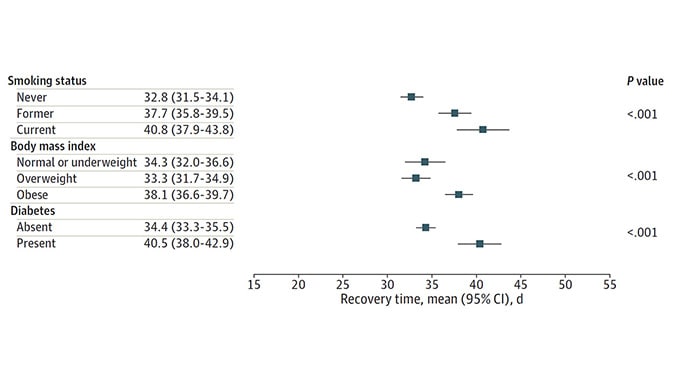
Recovery times were longer for smokers, those with diabetes, and those who were obese.
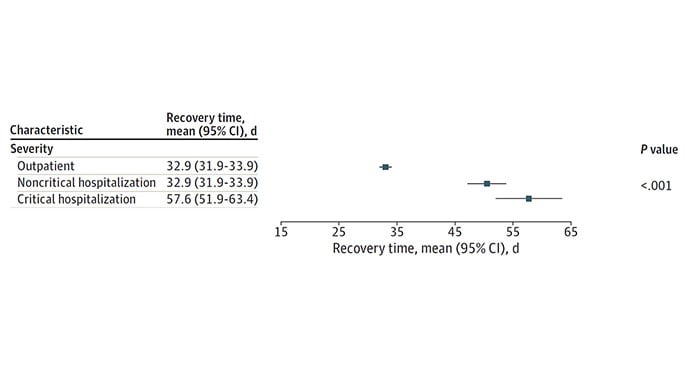
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.
Vaccination was associated with shorter recovery times, as you can see here.
This is all quite interesting. It's clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn't help us much with that.
Not that this was the authors' intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let's imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what's going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
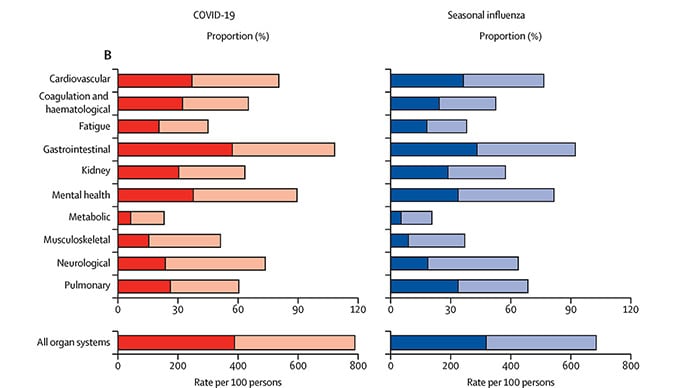
And what about other respiratory viruses? This study in TheLancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs Influenza. In general, the COVID outcomes are worse, but let's not knock the concept of "long flu." Across the board, roughly 50% of people report symptoms across any given organ system.
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it's bad; you've lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it's not random, it's really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I'm not saying that's what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale's Clinical and Translational Research Accelerator.
FCC Commissioner Brendan Carr slammed the Biden administration on Friday - writing on X that President Joe Biden has yet to connect a single American with high-speed internet.
"In 2021, the Biden Administration got $42.45 billion from Congress to deploy high-speed Internet to millions of Americans. Years later, it has not connected even 1 person with those funds. In fact, it now says that no construction projects will even start until 2025 at earliest," Carr wrote.
"Meanwhile, the Biden Admin has been layering a partisan political agenda on top of this $42.45B program – a liberal wish list that has nothing to do with connecting Americans. Climate change mandates, tech biases, DEI requirements, favoring government-run networks + more."
Carr is specifically slamming the Broadband Equity, Access, and Deployment (BEAD) program, which allocated $42.45 billion to support broadband infrastructure and adoption.
The program was established by the Infrastructure Investment and Jobs Act (IIJA), otherwise known as the so-called bipartisan infrastructure bill. The bill had no conservative victories and had many leftist carveouts, as Breitbart News detailed.
Congress passed the infrastructure bill in 2021, which would mean that the BEAD program has had little success in its two years since Biden passed the bill.
Transportation Secretary Pete Buttigieg also struggled to explain why Biden has only built “seven or eight” electric vehicle charging stations, which the funding also came from the IIJA.
“The timeline is bad. The policy cuts that the Biden Administration have made are even worse. The Biden Administration has set up a $42.45 billion program that is poised to miss the mark and leave rural communities behind,” Carr said in a statement to Breitbart News.
Carr continued, saying that the BEAD program fails to close the “digital divide,” or the gap between with those with high-speed internet and those without.
"The Biden Administration is barreling towards a broadband blunder. Congress has appropriated enough money to end the digital divide, but the Biden Administration is squandering the moment by putting partisan political goals above smart policy," Carr explained further. "It is doing so through rate regulation, through union, technology, and DEI preferences, and through a thumb on the scale for government run networks. All of this threatens to leave rural communities behind."
Intra-Cellular Therapies has secured another win with positive topline results from a Phase III study evaluating Caplyta (lumateperone) as an adjunctive therapy in patients with major depressive disorder (MDD).
In the trial, dubbed Study 502 (NCT05061706), a 42mg daily dose of Caplyta (lumateperone) as an adjunctive therapy provided a 4.5-point reduction on the Montgomery-Asberg Depression Rating Scale (MADRS) at week 6 compared to placebo, meaning the trial met its primary endpoint.
The drug also met the key secondary endpoint of change from baseline on the Clinical Global Impression Scale for Severity of Illness (CGI-S) at week 6.
The study randomised 480 subjects to receive 42mg Caplyta plus an antidepressant, or placebo plus an antidepressant to evaluate the efficacy and safety of the drug as an adjunctive treatment to antidepressants for patients with MDD.
Intra-Cellular’s share price leaped by 10.5% following the news.
Intra-Cellular has said that data from this trial along with that from the previously reported Phase III Study 501 (NCT04985942), forms the basis of a supplemental NDA (sNDA) submission for Caplyta as an adjunctive treatment for MDD. The submission is expected in the second half of 2024. Data from Study 501, which recruited 485 patients, showed a 4.9-point reduction in MADRS compared to placebo.
The MDD market is a competitive one with[MV1] several different players. The US Food and Drug Administration (FDA) approved AbbVie’s Vraylar (cariprazine) as an adjunctive treatment to antidepressants to treat adult patients with MDD in 2022. Vraylar generated $2.8bn in sales for AbbVie last year, as per the company financials.
Caplyta, a butyrophenone antipsychotic agent, is already indicated in adults for the treatment of schizophrenia and depressive episodes associated with bipolar I or II disorder, as both a monotherapy and an adjunctive therapy with lithium or valproate. According to GlobalData’s Pharma Intelligence Center, Caplyta is forecast to generate nearly $3bn in 2030, an increase from $918m in 2025.
GlobalData is the parent company of Clinical Trials Arena.
Sharon Mates, Intra-Cellular’s CEO said: “We are confident that the efficacy results from Studies 501 and 502, along with the favourable safety and tolerability profiles from these studies, will make lumateperone a drug of choice for patients suffering with MDD who are having an inadequate response to antidepressant therapy."
Ukrainian officials have already started preparatory work to organise a second peace summit, the Ukrainian president's chief of staff Andriy Yermak said on Tuesday, after the first conference led by Ukraine was held last weekend in Switzerland.
Yermak told an online press briefing late on Tuesday evening that the summit would only be possible after a joint plan had been figured out by member states, a process which he expected to take several months.
“The second summit will be possible when we have a joint plan,” he said, adding that a lot of work remained to be done.
A summit hosted by Switzerland over the weekend saw over 90 countries attend, but Ukraine and its allies failed to persuade major non-aligned states to join their final statement, and no country came forward to host a sequel.
Moscow was not invited to the event. Yermak said a Russian representative could be invited to the second such summit to be presented the peace plan decided upon by the event.
Russia launched a full-scale invasion of Ukraine in 2022, igniting the bloodiest conflict in Europe since World War Two. It has demanded Ukraine give up land and its ambition to join NATO in exchange for peace talks, conditions which Kyiv rejects.
Johnson & Johnson is facing a new proposed class action seeking damages and medical monitoring on behalf of women who have been diagnosed with cancer, or might develop it in the future, allegedly as a result of using the company's baby powder and other talc products.
The lawsuit, filed on Monday in New Jersey federal court, is the first to seek medical monitoring, or regular testing meant to catch cancer early, on behalf of talc users. The proposed class could include thousands of women, but would not include the more than 61,000 people who have already filed personal injury lawsuits over J&J's talc, claiming it contains cancer-causing asbestos.
J&J maintains its talc is safe, asbestos-free and does not cause cancer.
The law firms behind the new case are opposed to J&J's proposal to settle nearly all talc claims against it for $6.48 billion through a prepackaged bankruptcy. The same firms are also pursuing a separate class action seeking a court order blocking the bankruptcy.
The bankruptcy proposal needs support from 75% of talc claimants, with a three-month voting period ending on July 26.
Erik Haas, J&J's worldwide vice president of litigation, said in a statement that plaintiffs' lawyers brought Monday's "meritless" lawsuit to thwart the bankruptcy plan because they can collect more fees outside of bankruptcy, putting their own interests ahead of their clients.
"The plaintiff firms should cease the obstructionist behavior, and let their clients decide for themselves whether to accept the pending offer," he said.
Lawyers opposed to the deal have denied that they are motivated by higher fees and said the bankruptcy proposal would not adequately compensate their clients.
Chris Tisi, one of the lawyers bringing the new lawsuit, said in a statement that medical monitoring was necessary because the "inadequate funding" of the bankruptcy plan "doesn't realistically address the needs of women who could develop ovarian cancer in the future because of past baby powder use."
Both the proposed settlement and the new class action concern claims that talc caused ovarian and other gynecological cancers, which make up the vast majority of cases. A smaller number of claims have been brought by people who developed mesothelioma, most of which have settled.
J&J has already tried and failed twice to resolve current and future talc claims through bankruptcy.
The legal strategy, known as a Texas two-step, involves creating a subsidiary to absorb the company's talc liability, which then declares bankruptcy to settle the cases. The previous efforts failed because courts found that the new subsidiary lacked the "financial distress" to justify bankruptcy.