The White House met with Hunter Biden’s legal team just days before he defied a congressional subpoena, raising serious questions about coordination between the two camps, critics said.
The confab between Hunter Biden’s white-shoe attorney Abbe Lowell and Anthony Bernal, a top aide to First Lady Jill Biden, happened at 6 p.m. on Dec. 11, 2023, in the East Wing, according to White House visitor logs.
The logs also show Lowell met with President Biden, though it was likely in the context of a White House Hanukkah reception held on the same day.
Hunter Biden’s attorney Abbe Lowell made held a meeting with Jill Biden’s top deputy in December.AP
The Bernal-Lowell tête-à-tête took place just two days before Hunter Biden defied a House subpoena for a transcribed interview and caused a small frenzy at the Capitol by asserting his innocence at an impromptu press conference.
Biden Press Secretary Karine Jean-Pierre later admitted that President Biden had been “familiar” with what his son planned to say.
Hunter Biden ultimately came clean to House investigatorstwo months later.
A month before his meeting with Lowell, Bernal was also subpoenaed by the House Oversight Committee as part of their investigation into President Biden’s mishandling of classified documents.
Bernal, informally known as First Lady Jill Biden’s “work husband,” has become an infamous figure in the White House, where allegations of bullying and sexual harassment have circulated for years.
The aide — who has been with Jill Biden since 2008 — is widely considered untouchable because of his closeness to the first family.
What, if any coordination existed between Hunter Biden and the White House has long been shrouded in secrecy — but House Oversight Committee Chairman Rep. James Comer (R-Ky) told The Post the veil must be lifted.
“We’ve called on the White House to provide information about whether President Biden sought to influence or obstruct our investigation by preventing, discouraging, or dissuading his son from complying with the subpoenas for a deposition as part of the House of Representatives’ impeachment inquiry, but the White House has refused to provide any information,” said Comer.
“The White House must provide the public with information about the contents of this meeting in order to provide transparency to the American people.”
Jean-Pierre has repeatedly dodged inquiries on the subject.
“He’s a private citizen. He’s not a member of the White House. He doesn’t work here,” she said in January when asked about President Biden’s role in his son’s legal defense.
Reps for the White House insisted both of Bernal’s meetings stemmed from his attendance at the Hanukah reception — and insisted no Hunter Biden matters were discussed.
Thirty major central banks are expected to cut rates in the second half of 2024, a year when more than seventy nations will have elections, which often means massive increases in government spending. Additionally, the latest inflation figures show stubbornly persistent consumer price annualized growth.
In the United States, headline PCE inflation in February will likely grow by 0.4%, compared with a 0.3% rise in January, and consensus expects a 2.5% annualized rate, up from 2.4% in January. This is on top of the already 20% accumulated inflation of the past four years. Core inflation will likely show a 0.3% gain, according to Bloomberg Economics, which means an annualized 2.8%, building on top of the price increases of the past years.
Thirty central banks easing and seventy national governments increasing spending in an election year means more fuel for the inflation fire in a year in which money supply growth has bounced significantly from its 2023 lows.
Central banks ignored monetary aggregates when they shrugged off the risk of inflation in 2020, and now they are, again, easing way too fast when the battle against inflation has not finished.
Furthermore, the only real tool that central banks have used is hiking rates, because different parallel measures of money growth, including reverse repo liquidity injections, have kept money supply growth at an elevated rate even when the balance of the G7 central banks was moderating, albeit at a slower pace than announced.
Cutting rates may come too late because, by the time it is implemented, it will cause a double negative.
Government deficits will be cheaper to refinance, bloating an already record-high public debt yet again, but those cuts may have little impact on small and medium enterprises and families because they suffer significantly more from the accumulated effects of inflation, which means weaker margins, more difficulties to make ends meet, and impoverishment.
We must also remember that these persistent levels of official inflation come after relevant tweaks in the calculation of the consumer price index. We certainly know one thing: consumers do not pay attention to the annualized rate of growth in prices, but to the accumulated level of destruction of their purchasing power, and everyone, from Europeans to Americans, knows that they have become artificially poorer by the insane fiscal and monetary policies implemented in 2020.
Nobody who takes inflation seriously would even consider easing in an election year, adding trillions of dollars of deficit spending to the fire of inflation. Furthermore, the history of inflation warns us about giving up easily and too fast.
The Fed is making a big mistake by cheering the headline economic figures that come from disguising a private sector recession with a massive increase in public debt and weakening employment figures embellished by temporary jobs and public sector hiring. Additionally, it is making a mistake by giving dovish signals that make market participants take more risk. There has been no relevant reduction in the money supply if we include the different layers of liquidity injections. Announcing forthcoming rate cuts will certainly make speculative debt rise but will hardly change the credit demand from the backbone of the economy, small businesses, and families. Since the US government has rejected any calls for normalization and instead added more deficits and debt as if rising bond yields were not a problem, citizens and businesses have already suffered greatly from ongoing inflation and rate increases. As such, the rate cuts will help an already bloated government spending and the zombie corporations that keep access to capital markets. Everyone else will be hurt both ways, with inflation and lower access to credit.
You may think all the above problems are policy mistakes, but they are not. This is a slow process of nationalizing resources. Inflation and artificial money creation through deficits and monetization are a gradual transfer of wealth from real salaries and deposit savings to the government. You are basically becoming poorer to sustain an ever-increasing government size. The next time you read that massive deficits and monetary easing are good policies for the middle class, ask yourself why you find it harder each year to pay for goods and services. The mistakes made in 2020–2024 will cost the middle class many more taxes, even if the government promises it will only be “taxes on the rich,” the oldest gimmick to raise your taxes.
More taxes, persistent inflation, the hidden tax, and the loss of value of your wages. That is “easing” for you. A private sector recession with headline economic figures bloated by government debt. The recipe for stagflation.
Anesthesiology resident Max Feinstein, MD, discusses common medications used in anesthesia and their effects.
Following is a transcript:
Feinstein: Anesthesiologists sometimes tell patients that they are getting a "cocktail" of medications prior to their procedure, which can sound mysterious and intriguing, when in reality this cocktail is typically just comprised of a single medication called midazolam.
My name is Max Feinstein and I'm an anesthesiologist filming here at the Mount Sinai Hospital in New York City and in this video I demystify the medications that are administered to patients prior to procedures. If you find this video interesting or helpful, I'd really appreciate it if you liked it and subscribe to the channel. Let's dive in.
Before we get too far, just a quick reminder that this video does not contain medical advice; it's just a YouTube video. If you need medical advice, you should talk to your doctor.
Midazolam has several very important properties, which are why anesthesiologists use it. The first of those properties is anxiolysis, which is just a way of saying that it can reduce a person's anxiety. This is, of course, very helpful coming into the operating room if a person is nervous about getting surgery, which is very often the case for understandable reasons.
Another useful property of midazolam is that it can cause anterograde amnesia, meaning that patients won't remember anything after they have received the medication. There is an important distinction between anterograde amnesia, which means not remembering something after the medication has been administered, versus retrograde amnesia, which means not remembering something prior to the medication being administered. Midazolam only causes anterograde amnesia, and even then it doesn't necessarily cause amnesia in all patients. It can depend on the dose of medication that's given as well as patient factors like how much they weigh and whether they consume alcohol, which can have cross-tolerance with midazolam.
Midazolam can be used as a primary anesthetic in cases of light or moderate sedation where the goal is to have the patient still conscious and breathing on their own, but just very relaxed. Midazolam is also used frequently as a precursor to general anesthesia where a patient is completely unconscious and not aware of anything that's going on at all. The amount of midazolam that would need to be administered to produce a depth of general anesthesia is impractical in most cases, and so for that reason when patients do receive general anesthesia, there are other agents that are used such as propofol and sevoflurane.
In a small number of cases, there are other medications that can be administered either in lieu of or in conjunction with midazolam. One of those medications that anesthesiologists sometimes reach for is an opioid called fentanyl, which is also short-acting. Generally speaking, anesthesiologists like to reach for short-acting medications because that can help us maintain fine control over physiologic parameters like heart rate, blood pressure, and respiratory status.
When we do include fentanyl as part of the anesthesia cocktail, that's typically because the patient might be in pain and that might be the reason that they are coming in for surgery, for example, if they broke a bone. Anesthesiologists do have to use caution when mixing midazolam with opioids because together those can cause significant amount of respiratory suppression. If the plan is for the patient to undergo general anesthesia, where they're going to be intubated and mechanically ventilated, then respiratory suppression is kind of a moot point, but it is very important for patients to be able to breathe on their own in the time period immediately prior to undergoing general anesthesia.
Another medication that can be used as part of the anesthesia cocktail is a very low dose of propofol, which when given in 10 or 20 mg increments, won't produce general anesthesia in an adult but will actually just produce anxiolysis and perhaps a bit of amnesia. Having said that, propofol can irritate the vein where it's injected, which can be a reason to avoid giving more propofol to an awake patient than they need.
When I mentioned that midazolam is fast-acting, I mean onset can be 2 minutes or less when given through the IV. It typically won't last for more than an hour, although again that also varies depending on the patient. For adult patients, midazolam is typically administered through an IV, which is placed of course while the patient is completely awake. But for pediatric patients who won't tolerate having an IV placed while they are awake, then we can actually administer an oral form of midazolam, but it has a longer time of onset closer to around 20 minutes or so, again depending on the dose and the patient.
One of the common misconceptions around the anesthesia cocktail is that it's a sort of truth serum that causes patients to just blurt out their deepest darkest secrets. In reality, midazolam typically just causes patients to feel relaxed, chill out, maybe giggle a little bit about things that otherwise aren't that funny, and only extremely rarely do patients become disinhibited enough to start saying things that perhaps they wouldn't have said prior to receiving midazolam.
David: I... I feel funny. Is this going to be forever?
Feinstein: But honestly, I have never had a patient actually disclose anything really that embarrassing while they have been under the effects of midazolam or any other anesthetic agent. It's pretty uncommon.
I mentioned that some patients don't remember much, or anything, after they receive midazolam and I think it's really important for anesthesiologists to make patients understand that that may or may not happen once the medication goes in. Expectation setting is a really important part of the patient experience after all.
By the same token, I think it's very important for anesthesiologists to tell patients when they are receiving midazolam or any other medication that's going to change the way that they feel. I don't think it's really fair to surprise patients with medications through their IV without first telling them that they are about to get something that will change the way they feel. While the vast majority of patients who receive midazolam will feel pretty chilled out, there is a small proportion of patients who have what's called a paradoxical reaction where they become hyper-energetic after receiving the medication.
David's Dad: Stay in your seat.
David: [OUTBURST]
Feinstein: If you're a patient watching this video and you're wondering will you receive midazolam or any other medication as part of the anesthesia cocktail before your procedure, the answer is it depends.
Certain aspects of anesthesia practice can vary pretty considerably depending on factors like who your anesthesiologist is, what procedure you're coming in for, what medications and monitoring are available for patients prior to going into the operating room, and so forth. For these reasons, it wouldn't be surprising to me to know that a patient who is coming in for, say, a laparoscopic appendectomy at a certain hospital would probably not be offered midazolam unless there were extenuating circumstances. Whereas a different hospital that has different practice norms would routinely offer midazolam to patients who are coming in for the same procedure.
I do think this variation in practice begs an important philosophical question about the involvement that patients have with regard to the specific medications that they get for their anesthesia and also the extent to which anesthesiologists are involving patients in the decision about what medications will be administered.
On the one hand, I think there is a lot of benefit for anesthesiologists and their patients to have an open conversation about what medications will be administered and why, but then on the other hand that's also not entirely feasible, especially if a patient is under general anesthesia. And there is also an argument to be made for the fact that it can be overwhelming for patients to have to make medical decisions about the specifics of exactly what they are receiving as part of their anesthetic plan that might overall make the experience more anxiety-inducing than it needs to be, as opposed to simply leaving the decisions to the anesthesiologist about how best to produce the outcome that the patient desires, for example, feeling relaxed or being completely unconscious for a procedure.
If you are a patient and you do have any questions or concerns about any part of your anesthesia plan, then it's important to bring it up with your own physician before you undergo your procedure.
Max Feinstein, MD, is a PGY-4 anesthesiology resident at the Mount Sinai Hospital in New York City, where he is also chief resident of teaching. His YouTube channelopens in a new tab or window focuses on perioperative medicine, especially the role of the anesthesiologist.
Thames Water parent failed to make payments on a bond
CCC bond spreads have reached euro region crisis levels
The junkiest corporate debt is becoming increasingly hazardous for investors amid mounting signs that a default cycle is picking up steam.
The holding company of Thames Water Ltd. this week failed to make payments that had come due on a £400 million bond ($504 million). It follows a plunge in the bond prices of Altice France last month after management told investors they would have to participate in “discounted transactions” to help the firm slash its debt.
One in seven women will die within 2 months of being diagnosed with ovarian cancer, anew reportfrom the United Kingdom states. But if diagnosed at the earliest stage, 9 in 10 women will survive. Two thirds of women are now diagnosed late, when the cancer is harder to treat.
Diagnosis is difficult for many reasons, among them that women sometimes think symptoms are a natural part of menopause and don't acknowledge or report them. Clinicians may mistake abdominal symptoms for those of a bowel condition or bladder problem. Almost half of GPs (46%) in the United Kingdom mistakenly believe that ovarian cancer symptoms present in only the later stages of the disease.
Cervical Test Doesn't Detect Ovarian Cancer
Additionally, there are misconceptions regarding cervical cancer screening — one study found that "40% of women in the general public mistakenly believe that cervical screening detects ovarian cancer." But there is no current screening program for ovarian cancer in the United Kingdom or United States.
During a pelvic exam, the physician feels the ovaries and uterus for size, shape, and consistency and that can be useful in finding some cancers early, but most early ovarian tumors are difficult or impossible to feel, the American Cancer Society notes.
Recognizing the Red Flags
Victoria Barber, MBBS, a general practitioner in Northamptonshire and a Primary Care Advisory Board member with the Target Ovarian Cancer program in the United Kingdom published a paper in the British Journal of Nursing (2024 Mar 7. doi: 10.12968/bjon.2024.33.5.S16) on the program's efforts to urge clinicians to recognize ovarian cancer red flags and to "never diagnose new-onset irritable bowel syndrome or overactive bladder in women over 50 without ruling out ovarian cancer."
She says nurses should be involved to help with earlier diagnosis of ovarian cancer as they are often involved in evaluating urine samples. Nurse practitioners, she notes, are typically included in consultations for abdominal symptoms and potential urinary tract infections.
"If the woman is recurrently presenting with urinary symptoms, sterile midstream urine samples should raise alarm," she says. "The woman may have diabetes, an overactive bladder, or interstitial cystitis; however, urgency and frequency are some of the symptoms of ovarian cancer, and they need investigation."
Persistent Systems Over Age 50
The paper lists ovarian cancer symptoms from the UK's National Institute for Health and Care Excellence and notes that among red flags are having any of the following persistently/frequently (particularly more than 12 times per month and especially if the woman is 50 years or older):
Ernst Lengyel, MD, PhD, UChicago Medicine's Chairman of the Department of Obstetrics and Gynecology in Chicago, Illinois, who was not involved with the paper, said the situation in the United States is similar to that described in the United Kingdom.
"The diagnosis is delayed because the symptoms are unspecific. The problem is that ovarian cancer is so rare, and primary care physicians or nurse practitioners have to consider over 100 differential diagnoses," he says.
In the United States, he says, it is likely easier to get in and see a physician because of the private insurance options and because there are more gynecologic oncologists in large urban areas. Getting imaging approved — such as ultrasound and computed tomography scans — is also easier in the United States.
Still, "there is no effective way to diagnose ovarian cancer early," he says. "No single test or combination of symptoms can be used as a screening test."
The CA-125 blood test measures proteins that can be linked with ovarian cancer, but is not a screening test, he notes.
"Large UK and US studies have not been able to show a survival benefit with ultrasound, serial CA-125, or a combination thereof," Dr Lengyel said.
Weight Gain May Also Be a Sign
A broad range of clinicians should be aware of the symptoms the author mentions, he says, especially primary care physicians, nurse practitioners, and obstetrician/gynecologists.
"Too often, symptoms that women report are ignored and treated as unspecific or psychosomatic," Dr Lengyel says. "It is easy to disregard recurrent complaints and move on instead of being vigilant and working them up. Ironically, women with ovarian cancer can initially gain weight, which is counterintuitive as most doctors believe that patients with cancer lose weight. However, if they develop abdominal fluid, a patient often gains weight."
Dr Barber and Dr Lengyel reported no relevant financial relationships.
A principal goal of Stark Realities is to “expose fundamental myths across the political spectrum” — and few myths are as universally embraced as the notion that US participation in World War II lifted the American economy out of the Great Depression.
This myth is dangerous not only because it leads citizens and politicians to see a bright side of war that doesn’t really exist, but also because it helps foster a belief that government spending is essential to countering economic downturns. That belief, in turn, has helped propel us to a point where the national debt now exceeds $34.6 trillion, with interest payments alone on pace to reach $1 trillion a year in 2026, inviting financial catastrophe
In part, the wartime-prosperity myth springs from the fact that, during conflict on the scale of World War II, broad, macroeconomic measures like gross national product (GNP) and the unemployment rate are completely untethered from the economy’s most important facet: the standard of living enjoyed — or endured— by everyday people.
Between 1940 and 1944, real GNP rose at an unprecedented 13% annual clip. Using GNP alone, one would think the war delivered a major improvement in the standard of living, with Americans enjoying a greater abundance of goods, accompanied by a rise in quality, selection and affordability.
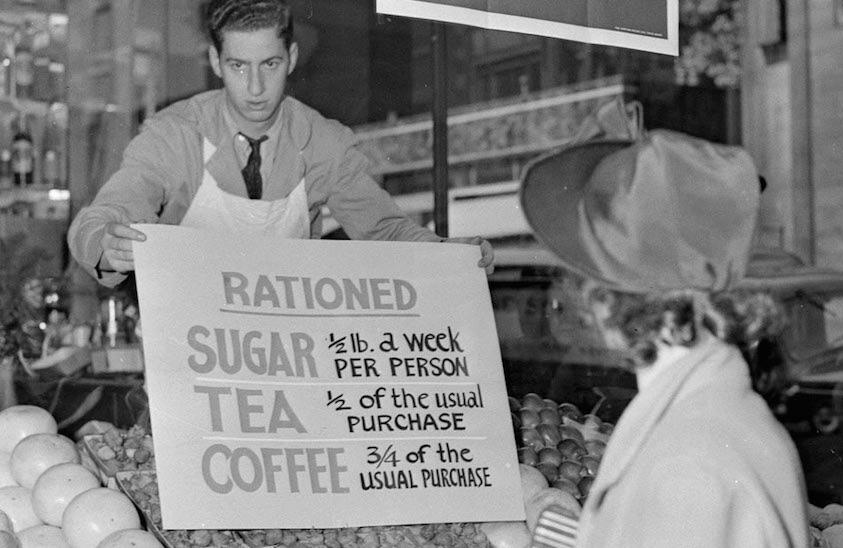
The reality was the exact opposite: Americans endured rationing, shortages, declining product quality, and the outright unavailability of many new goods, such as cars, trucks and stoves. This was the inevitable result of factories and raw materials being redirected from the creation of things consumers want to building things like tanks and fighter planes that do nothing whatsoever to improve people’s lives (setting aside the separate issue of the war’s justness).
In many respects, America experienced an outright economic devolution. In the preceding century, industrialization and the division of labor led to enormous increases in productivity. During World War II, however, shortages motivated people who’d contentedly relied on farmers to start growing their own food and canning it. The scarcity of new clothing led homemakers to redirect time and energy to sewing their own garments and resewing them to stretch as much use out them as possible.
“Those remaining on the home front were forced to produce for themselves what they had previously been able to purchase,” wrote Steven Horwitz and Michael J. McPhillips. “The household again became a center of production rather than consumption alone.”
GNP wasn’t the only measure falsely signaling wartime prosperity; employment numbers from the era were likewise misleading. The US unemployment rate plummeted from 17% in 1939 to 1.2% in 1944. Note, however, that military service members are not considered part of the labor force — which means that the draft extracted 11.5 million men from the denominator in the unemployment rate calculation.
Another 6.3 million volunteered, though many signed up because they preferred to secure a role they favored rather than face the chance of being drafted as an infantryman.
While it’s true that draftees and volunteers were “employed” by the armed forces, all these millions of men — no matter how noble their overseas missions may have been — weren’t doing anything to create prosperity at home.
Not a prosperous path to full employment: Soldiers under withering fire on D-Day’s Omaha Beach
That’s not to say the war machine didn’t demand laborers. With so many able men taken out of the economy, the slack was taken up by teenagers, women and retirees, many who’d have preferred to be doing other things.
In a growing economy, more people are producing goods and services, and elevating standards of living in the process. That was far from the case during World War II. Factories were humming, but they were making bayonets, bombs and battleships. “Four-tenths of the total labor force was not being used to produce consumer goods or capital capable of yielding consumer goods in the future,” noted Robert Higgs.
Defying conventional wisdom about “wartime prosperity,” Americans’ standard of living suffered tremendously from their government’s entry into World War II. In The Reality of the Wartime Economy, Horwitz and McPhillips tapped some interesting source material to bring the grim economic realities of American life during World War II into sharp focus.
For example, a series of newspaper ads placed by Canton Electric Light & Power Company — a local New York State utility — present a vivid, time-lapse portrayal of rapidly declining conditions following the December 1941 declaration of war:
Foreshadowing anticipated shortages, a March 17, 1942 ad for appliances is headlined “You Can Still Buy Them.” The ad includes a qualifier that’s upbeat while still signaling creeping scarcity: “We have a fairly good supply.”
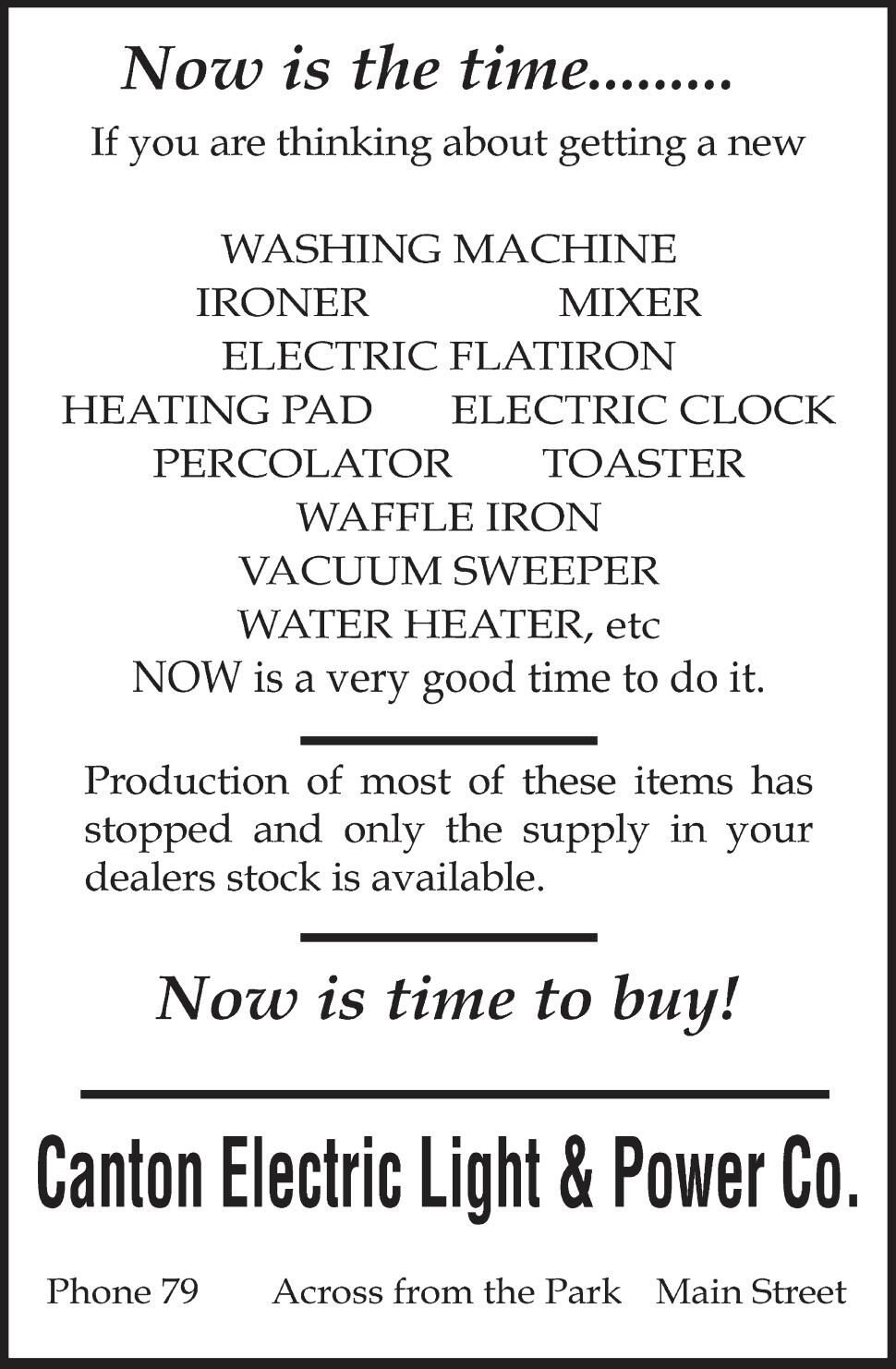
Just two months later, Canton Electric’s ad says “Now Is The Time” to buy various appliances and equipment, warning that “production of most of these items has stopped and only the supply in your dealers’ stock is available.”
Another two months later, a July 1942 ad indicates that some items that were briefly not available are back in inventory.
In November of that first year of America’s World War II participation, Canton Electric switched to warning consumers that, “due to the war emergency, it is quite impossible to get replacement motors for civilian use,” and urging them to ensure they’re properly maintaining their “stokers and oil burners.”
Later that same month, Canton Electric punted on advancing its retail business altogether, instead using its ad space to encourage readers to grow their own food, eat everything on their plates and comply with ration-stamp rules.
Horwitz and McPhillips also drew on letters written between 1942 and 1945 by Saidee Leach to her son serving in the Pacific. Contrary to the image of prosperity supposedly indicated by leaping GNP or plummeting unemployment, she tells him of:
Conserving scarce home-heating fuel during the coldest days by wearing fur coats indoors and residing only in their kitchen
Having her typewriter seized by the government, and now using a lesser model she acquired from a Howard Johnson “which had to close due to the ban on pleasure driving.”
Making an Easter dinner centered on fried Spam, because she “could not get fresh meat of any kind,” and later noting that “potatoes have entirely disappeared”
Local farmers refusing to sell their turkey flocks for Thanksgiving meals at the prices set by the Office of Price Administration — illustrating the folly of government price controls.
That is not the picture of an economy delivered from the Great Depression. Rather, “World War II institutionalized the falling standards of living of the depression through wage and price controls, and extensive rationing of consumer goods and services,” wrote Peter Ferrara. “The economic deprivation, and reduced standards of living, continued, although people perceived it was now for a good cause.”
America’s postwar experience presents another pointed contradiction of the myth of wartime prosperity.
As the war’s end grew closer, Keynesian economists unanimously predicted peace would bring economic disaster. For example, Paul Samuelson said America would experience “the greatest period of unemployment and dislocation any economy has ever faced.”
Alvin Hansen warned that the economy must be kept on a centrally-controlled wartime footing, even in peacetime: "When the war is over, the government cannot just disband the Army, close down munitions factories, stop building ships, and remove all economic control.”
Nobel Prize winner Paul Samuelson, who predicted peace would bring economic disaster, taught Nobel laureate Paul Krugman, who predicted the internet's impact would be akin to that of the fax machine
However, that’s pretty much what happened — and Hansen, Samuelson and their fellow economic flat-Earthers couldn’t have been more wrong about the consequences. “The year 1946, when civilian output increased by about 30 percent, was the most glorious single year in the entire history of the U.S. economy,” wrote Higgs.
This despite the fact thatgovernment purchases of goods and services collapsed by 68% between the second quarter of 1945 and the first quarter of 1946 — and upwards of a million civilian government employees were laid off and millions of service members discharged.
As war-fighting men poured back into civilian life, millions of women withdrew from the labor force, contentedly returning to duty as mothers and home managers. Rather than soaring as predicted by the “experts,” unemployment merely edged higher, from 1.9% in 1945 to 3.9% in 1947.
“Less than a year and a half after VJ-day,” crowed President Truman, “more than 10 million demobilized veterans and other millions of wartime workers have found employment in the swiftest and most gigantic change-over that any nation has ever made from war to peace.” (Note this happened despite — and in part because of — Truman’s failure to institute a higher minimum wage as the war ended.)
Having been proven enormously wrong about the economic implications of peace, Keynesians scrambled to credit the war with enabling the postwar boom, arguing that it was fueled by people drawing down savings accumulated while the supply of consumer goods was sharply restricted. However, as Higgs determined by studying the data of the time, “Holdings of liquid assets did not decline at all after the war. People financed their spending for consumer goods by reducing their saving rate.”
Once again an engine of real prosperity: In 1946, vehicles proceed along Ford’s first postwar assembly line (Ford Motor Company Archives)
Contrary to the myth, it was only after World War II that — free from the government’s commandeering of factories, workers and resources, and saddled with fewer price controls and other federal market intrusions — America was finally able to emerge from the Great Depression.
You wouldn’t know that if you evaluated the economy’s health using Keynesians’ preferred measure. Just as the GNP gauge provided a 180-degree misreading of wartime economic realities, it failed in similarly spectacular fashion during the postwar boom: From 1945 to 1947, GNP plummeted 22%.
In addition to further illuminating the shortfalls of aggregate economic measures, America’s postwar economic experience delivered another broadside to the myth of World War II-fostered prosperity, and to the idea that government spending, central planning and market interventions are essential to economic achieving economic recovery.





{kind=link}
{kind=link}
{kind=link}